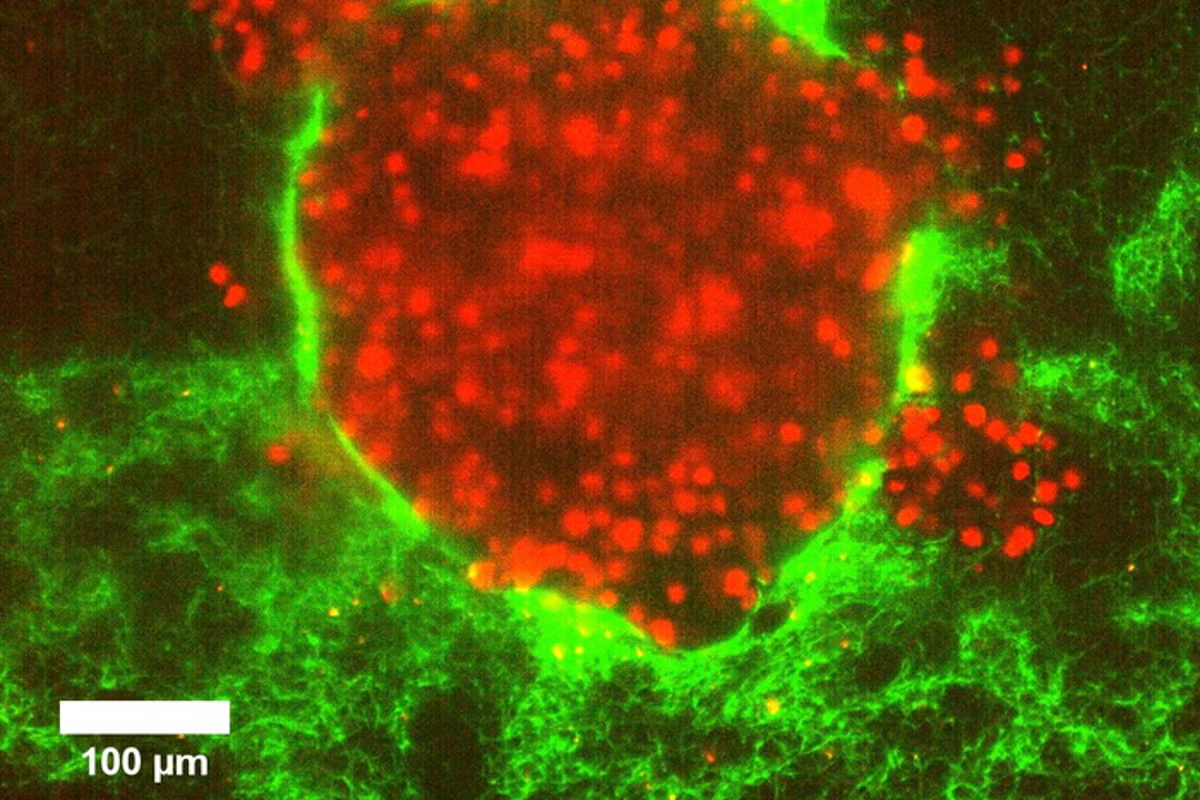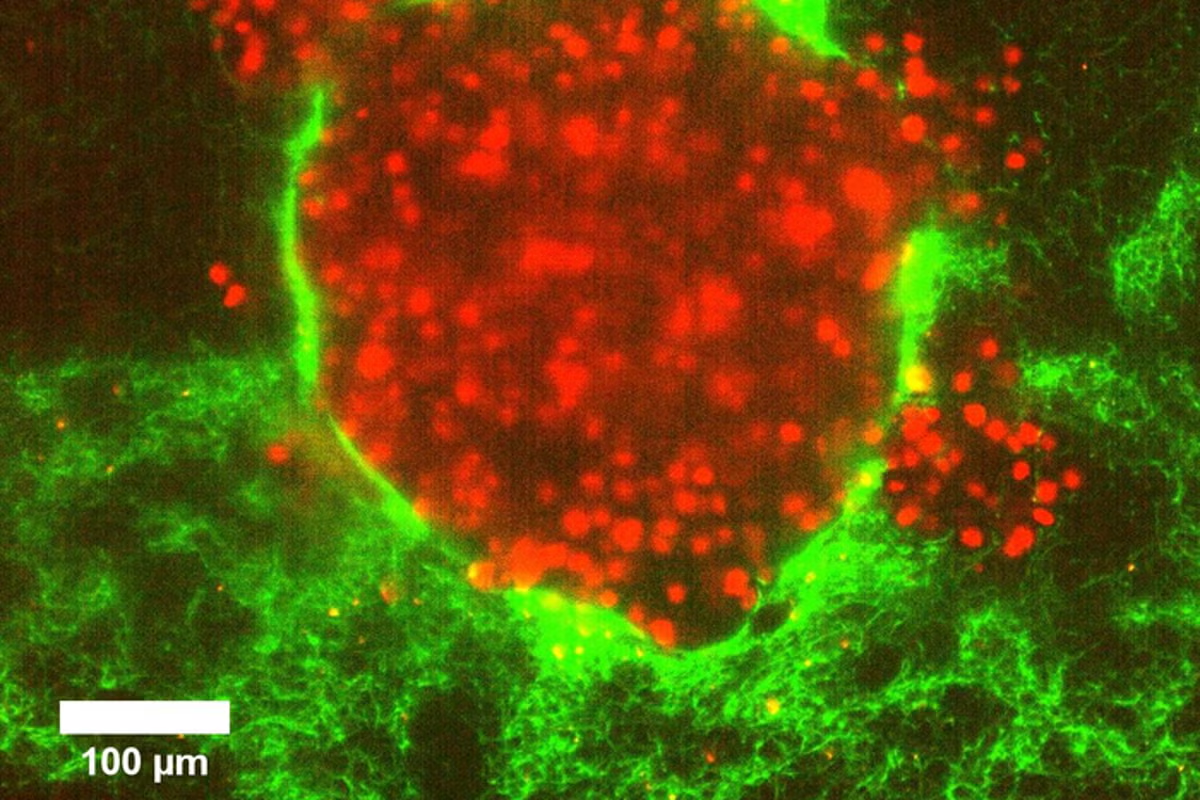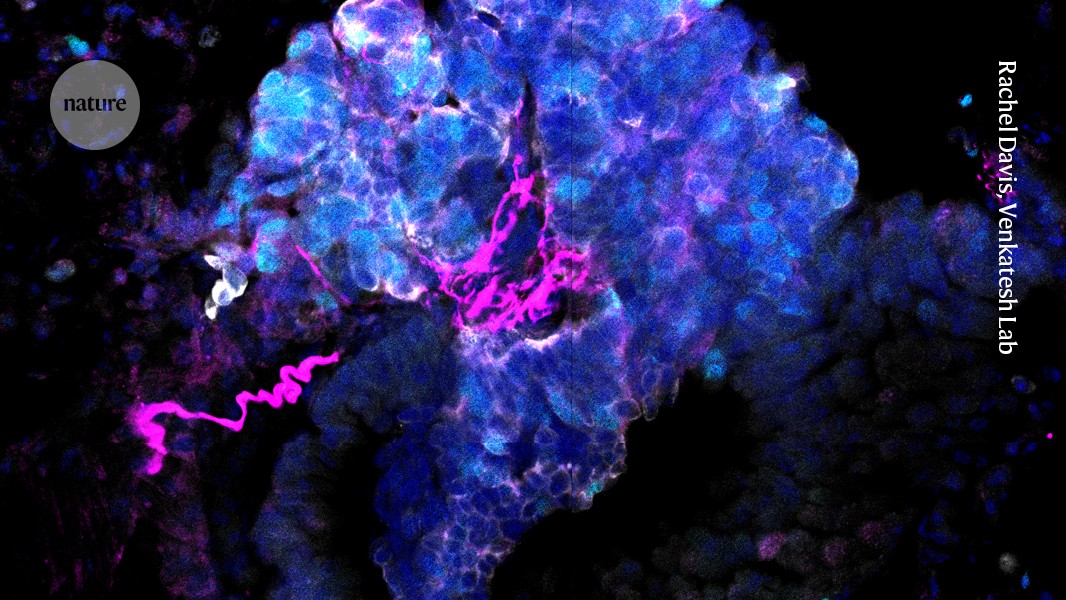
Neurons (magenta) innervate a small cell lung cancer tumour.Credit: Rachel Davis, Venkatesh LabAt first, Filippo Beleggia had no interest in neurons. A cancer biologist studying small-cell lung cancer (SCLC), he deployed a sophisticated screening technique to search for genes that drive tumour progression in a mouse model of the disease. Although it accounts for only around 15% of lung cancers, SCLC is the most aggressive and metastatic form of the disease and has limited options for treatment. Beleggia was hoping to identify genes involved in processes such as cell division or responses to DNA damage, and says his aim was to discover genes “that we could then build therapies on”.What this first screen delivered, however, was a list of genes implicated in neurobiology. Such was the surprise, Beleggia says, that his team dismissed it as an artefact of the technique they had used.Nature Outlook: Lung cancerIt was known that a high fraction of cells in SCLC tumours resemble neuroendocrine cells — with the lung’s native neuroendocrine cells being the suspected origin of these tumours. Given that such cells release hormones or neurotransmitters and express a handful of neuronal markers. Beleggia saw the result as a “by-product of this neuroendocrine differentiation”, adding that the phenomenon “doesn’t really have any relevance for the cancer state”.He and his colleagues at the University of Cologne in Germany therefore ran a second large-scale screen, then a third. One screen looked for genes that are most often mutated in human SCLC tumours. The other identified the genes most abundantly expressed in SCLC tumours compared with other cancers and in healthy tissues. The techniques were different, but the results were the same — the top hits were dominated by genes with neuronal functions.What struck Beleggia in particular was that many of these genes were involved in the assembly and maintenance of synapses — the cell-to-cell junctions across which neurotransmitters travel to allow neurons to regulate their targets. “This was completely unexpected,” he says.Working with neuroscientist collaborators, Beleggia showed that SCLC cells form true synapses with neurons. Their paper was published last September1, alongside a study by US researchers who had made the same discovery2.The US study was led by Michelle Monje, a neuro-oncologist at Stanford University in California, and Humsa Venkatesh, a cancer biologist at Harvard University in Cambridge, Massachusetts, and one of Monje’s former postdocs. They had previously shown that primary brain tumours are intimately regulated by interactions with neurons. Wanting to know how common it is for cancers to be directly influenced by neurons, Venkatesh suggested that they look at cancers that metastasize to the brain. SCLC was an obvious choice. “Lung cancer actually represents the most common brain cancer,” says Monje.The finding that neurons form synapses with SCLC cells was a surprise. But more important for the development of fresh treatments was the demonstration that synaptic input accelerates SCLC progression.Each group showed that, in mice with SCLC, drugs that reduce synaptic signalling slowed the disease. The findings, Monje says, “open up a new realm of potential helper medicines” to treat SCLC.A brain-loving cancerBoth groups sought advice from Stanford oncologist Julien Sage, who has studied SCLC for around 20 years. “Small-cell lung cancer is the most aggressive type of lung cancer,” Sage says. “It is the one that grows the fastest, the one that is the most metastatic.” It’s also the deadliest, he adds. “The five-year overall survival is still below 10%. And it’s a disease that just loves going to the brain.”Treating metastatic disease is therefore central to managing SCLC. Roughly one in five people already have brain metastases when diagnosed with SCLC, up to 80% of people with SCLC develop brain tumours eventually.Sage says this propensity, plus its neuroendocrine features, made SCLC “a natural cancer to potentially connect to the neural system”. Since the mid-2010s, his work has moved in that direction. In 2019, his group showed that cellular protrusions resembling neuronal axons aid the migration and metastasis of these cancer cells3.Then, in 2023, the team showed that when SCLC cells enter the brain, they can communicate with astrocytes — glial cells known for their mutualistic relationship with neurons4. In the cancer cells, this signalling induces genetic programs resembling those seen in brain development, promoting tumour growth in the brain. “In an environment where cancer cells can have friends, then it’s just easier for the cells to grow,” Sage says.Now, the latest synapse studies say that neurons, as well as astrocytes, are friends to SCLC.In February last year, Leanne Li, a cancer biologist at the Francis Crick Institute in London, revealed more details of how SCLC cells that develop neuron-like characteristics can drive tumour aggressiveness. Li’s group first confirmed that the neuroendocrine-like SCLC cells can fire action potentials — the distinctive electrical spikes by which neurons encode information. She then revealed that neighbouring non-spiking, non-neuroendocrine SCLC cells metabolically support spiking cells in ways remarkably reminiscent of how astrocytes assist neurons5.Li also found that the neurotransmitter acetylcholine makes the neuroendocrine SCLC cells fire more frequently. This was interesting for three reasons. First, cigarette smoke — the main cause of SCLC — contains nicotine, which mimics acetylcholine’s excitatory action on these cells. Second, the vagus nerve innervating the lungs releases acetylcholine. And third, studies have shown that neuroendocrine SCLC cells can release acetylcholine. Li therefore thinks that smoking or the vagus nerve might promote early cancer growth by increasing electrical activity, before what she calls a “self-propagating loop” takes over.To test the importance of this electrical activity, Li genetically modified cancer cells so that a drug or light could change their excitability. When excitability was decreased, tumour growth slowed; when it was increased, tumours grew quicker. “You can really alter the tumour phenotype of these cells both in vitro and in animals,” Li says.Combined, the Beleggia and Monje synapse studies showed definitively that when SCLC cells are present in the brain, neurons synapse onto them. Beleggia’s research also provided evidence of synapses on cancer cells in the lungs.Some synapses formed with brain neurons used the excitatory neurotransmitter glutamate. Others used GABA, which mainly inhibits neurons — but owing to the ionic concentrations in SCLC cells, this too was excitatory.The finding that synaptic excitation drives cancer progression was first demonstrated by growing cancer cells in a dish with and without neurons present. When neurons were present, the cancer cells divided faster. Applying various drugs indicated that this growth-promoting effect came mainly from synaptic connections. Monje and Venkatesh also stimulated synaptic input into cancer cells grafted into a mouse’s brain, confirming that synapses increase cancer proliferation in this setting — a phenomenon that probably speeds up the development of metastatic brain tumours.Monje and Venkatesh also looked at the influence of the vagus nerve in a mouse model of primary lung tumours. The researchers found that there was no effect if they cut the vagus nerve once a tumour was already established. Removing the nerve when tumours were still in early development, by contrast, hugely delayed their emergence.Venkatesh says they are now investigating the mechanism underlying this effect. She says it suggests that nerves either directly modulate early-stage cancers or create a permissive environment for tumour initiation. Subsequently, tumours become more autonomous, potentially with Li’s self-propagating loop in play.However, the long-held view of SCLC as arising from neuroendocrine cells in the lungs has been challenged. Trudy Oliver, a cancer researcher at Duke University in Durham, North Carolina, has proposed that the main cells of origin are, in fact, the lung’s basal cells6. Unlike a healthy lung’s native neuroendocrine cells, basal cells aren’t innervated. Consequently, Oliver questions whether tumours stemming from basal cells would have the same early reliance on the vagus nerve.Venkatesh says that the cell of origin could be one of many candidates. But regardless, she adds, there’s abundant evidence of a neuronal link. A SCLC tumour “has the receptors, has the machinery, has all of these abilities to be able to integrate with nerves and receive these neural cues”, she says.Helper medicinesTargeting neural mechanisms could potentially augment existing chemo-, radio- and immunotherapies for SCLC. But this is unlikely to be a cure. “I’m not sure whether neuromodulation alone is going to kill the tumour,” Beleggia says, “but it can slow it down.”In both his and Venkatesh and Monje’s studies, a clinically approved drug that inhibits neural activity was given to mice that were engineered to develop brain tumours made of SCLC cells. Beleggia used riluzole, a drug for treating motor neuron disease; the US team chose the epilepsy medication levetiracetam. Both drugs slowed tumour development.“The good thing,” says Beleggia, “is that there are already a lot of drugs that are safe” and that target neurons and synapses.Monje thinks that trials to assess the effects of such drugs should be straightforward to establish, because the drugs already have regulatory approval. There’s also the possibility of retrospectively analysing clinical data to ask whether people with SCLC who happened to be taking neuron-targeting drugs, such as antidepressants or anti-seizure drugs, fared better than people not taking them. Positive results could lead physicians to repurpose these medications for people with SCLC.Studies of neurons influencing SCLC could also change what other drugs are prescribed to people with the disease. For example, when people with SCLC and brain metastases develop epilepsy, they’re often given drugs that augment the activity of GABA. But this normally inhibitory neurotransmitter excites the cancers. “It may help the seizures,” Venkatesh says, “but it’s going to make the tumour worse.” Prescribing anti-seizure drugs with alternative mechanisms of action could therefore avoid accelerating tumour growth.And Monje thinks that the neuroscience of lung cancer could spur the development of wholly new drugs aimed at fresh targets. If scientists can uncover, for instance, the signalling pathways through which electrical activity accelerates cellular division, fresh therapeutic targets might be revealed.“This research is in its early stages,” says Venkatesh. She concedes that it’s uncertain whether neural mechanisms will provide potent ways to treat advanced lung tumours. But if synaptic inputs, or the neuronal features of these cells, prove to be key to how these cancers establish themselves in the brain or any secondary site, then inhibiting them could slow or prevent metastatic disease.“If we can do that,” Venkatesh says, “I think that’s a win.”
How the connection between lung cancer and the brain could lead to better treatments
The discovery that small cell lung cancer has several neuronal features is yielding biological insights that could ultimately save lives.
1,701 words~8 min read