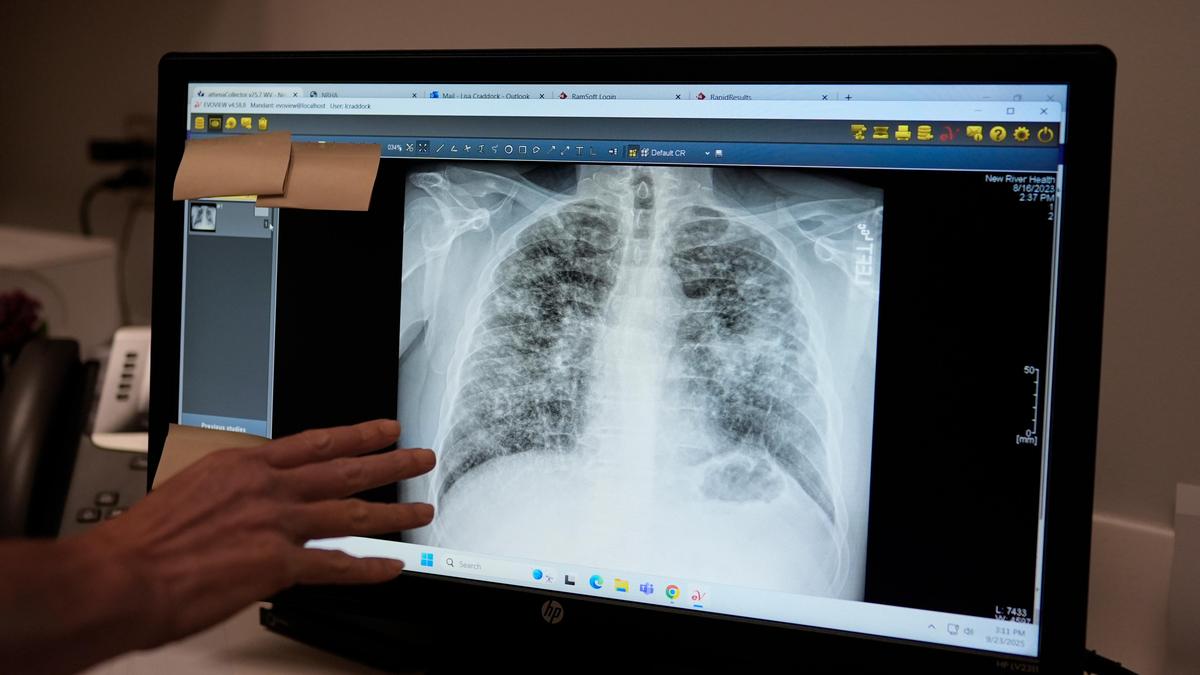
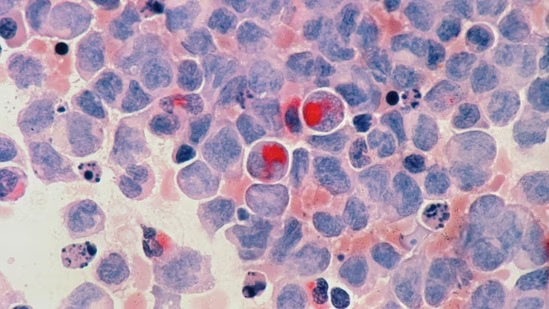
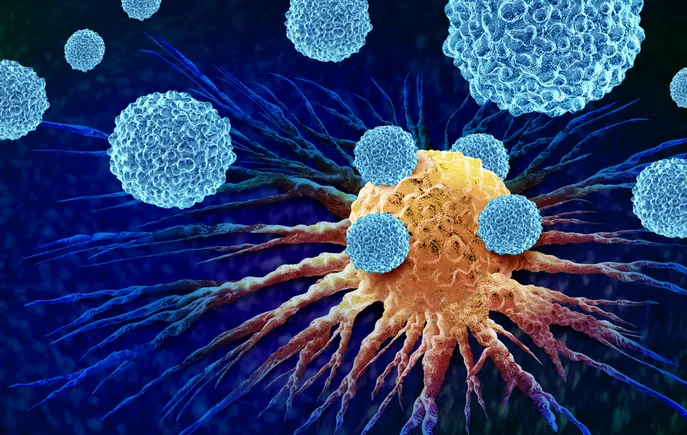
Immunotherapy targets cancer by boosting the immune system’s response to malignant cells.Credit: Garo/Phanie/Science Photo LibraryImproving survival with immunotherapyEven after a lung tumour has been surgically removed, many patients relapse. Immunotherapy is being explored as a way to reduce the risk of relapse. Previous trials have shown that immunotherapy given before surgery can drastically shrink tumours, but long-term studies are needed to determine whether this strategy also results in fewer cases of relapse.Nature Outlook: Lung cancerA phase III trial led by Patrick Forde at Trinity College Dublin begins to fill that gap. The team recruited 358 people with non-small cell lung cancer — the most common form of the disease — whose tumours were surgically removable. Each person was randomly assigned to receive chemotherapy alone or in combination with the immunotherapy nivolumab. After treatment, all patients underwent surgery. At the end of five years, 65% of participants who received nivolumab plus chemotherapy were still alive, compared with only 55% who received chemotherapy alone.The researchers also searched trial data for biomarkers that might predict outcomes. They found that almost every person whose tumour was completely wiped out before surgery was still alive at the five-year mark, compared with only 56% of those who still had detectable cancer cells. Forde’s team also examined circulating tumour DNA (ctDNA) in the blood. Three-quarters of participants whose blood tests revealed no ctDNA before surgery survived the study period, compared with about half of those whose tests confirmed the presence of ctDNA. These markers might serve as early predictors for gauging treatment outcomes.N. Engl. J. Med. 393, 741–752 (2025)More-effective screening Many lives can be saved by using low-dose computed tomography (CT) scans to screen for lung cancer. Screening typically focuses on people aged 50 or older who have a history of heavy smoking. However, there is growing evidence to suggest that offering screening on the basis of a wider set of criteria that influence lung cancer risk might identify people in need of treatment more effectively.A team led by Jens Vogel-Claussen at Charité University Medicine Berlin compared people selected using conventional criteria based on smoking history with those selected with a risk-prediction model that takes account of other factors, such as family history of lung cancer.The researchers screened nearly 5,200 people who met one or both criteria, and identified 111 cases of lung cancer. Significantly more lung cancers were detected in the risk-prediction group (97%) than in people selected using the conventional approach (77%). Use of the model also resulted in fewer people needing to be screened to detect a single case of lung cancer, with lung cancer detected in about 1 in every 39 people, compared with 1 in every 46 people for the conventional approach. The findings indicate that screening programmes could be more effective if countries adopted individual risk models rather than focusing only on smoking.Lancet Oncol. 26, 1541–1551 (2025)Identifying hidden patterns Lung adenocarcinoma, the most common form of non-small cell lung cancer, looks and behaves differently from person to person across ethnic groups. Interactions between genomics, specific tumour mutations and proteins, and environmental exposure to carcinogens seem to drive these differences. A greater understanding of how these factors increase the risk of lung adenocarcinoma could therefore help researchers to design better treatments tailored to individuals’ biology.Most molecular analyses of lung cancer have included sample sizes that are too small to tease out potential underlying differences by race, ethnicity, sex and environmental exposure. Shankha Satpathy at the Broad Institute of MIT and Harvard in Cambridge, Massachusetts, and his colleagues tried to address this gap by analysing genes and proteins from 406 lung adenocarcinoma tumours collected from people with diverse backgrounds. They also gathered normal, tumour-adjacent tissue samples from the participants.The team identified four main groups of carcinogens, defined by mutational signatures that were implicated in lung adenocarcinoma. The clearest signatures involved carcinogens linked to tobacco smoke and air pollution. Another signature appeared in a specific group: Asian women who had never smoked. This signature might be caused by nitrosamines, a class of cancer-causing chemicals found in processed food, cosmetics and tobacco smoke. People with carcinogen-associated signatures had worse survival outcomes than did those in other groups.The scientists also made a surprising finding in relation to the seemingly healthy tumour-adjacent tissue. In people with carcinogen-associated signatures, this tissue showed signs of chronic inflammation, altered metabolism and carcinogenesis. This indicates that carcinogen exposure might create a broadly hospitable environment for cancers to form in tissues, rather than triggering single point mutations.According to the authors, the results point to the importance of considering a person’s exposure history, as well as their specific tumour’s genetics, when designing treatment protocols. Their findings could lead to the identification of biomarkers for subtypes of lung adenocarcinoma.Cancer Cell 43, 1731–1757 (2025)New option for hard-to-treat casesMutations in the gene encoding the epidermal growth factor receptor protein (EGFR) account for up to 15% of lung cancer cases in Western countries and up to 50% in East Asian populations. Therapies targeting this mutation have had success, but many patients eventually develop resistance, leaving them with limited treatment options. A new drug with an entirely different mechanism could soon offer an alternative for such patients.EGFR is a cell-surface protein that receives signals and translates them into instructions that promote cell growth and division. When mutated, EGFR can get stuck in the ‘on’ state, causing it to drive cells to proliferate out of control. Most therapies that target EGFR aim to block its signal to cells, but Wenfeng Fang at Sun Yat-Sen University Cancer Center in Guangzhou, China, and her colleagues are trialling a drug that delivers chemotherapy directly to tumours by way of a highly expressed surface protein, Trop-2, that occurs in EGFR-mutated cells. The drug, called sacituzumab tirumotecan, uses an engineered antibody that seeks out Trop-2 and carries a potent chemotherapy drug that it delivers directly to cancer cells through the targeted protein. After the antibodies attach to their protein targets, they are taken up by the cancer cell and, once inside, release their toxic payload, sparing healthy surrounding tissue.In a phase III trial, the team recruited 376 patients across 66 sites in China whose cancer had already progressed after EGFR-targeted therapy. Half of the participants received the new drug and the other group received standard chemotherapy — the usual next step after targeted therapies fail. A year and a half after receiving treatment, the group given sacituzumab tirumotecan was faring significantly better. People in this group experienced a median of eight months without their cancer getting worse, compared with four months for those who received standard chemotherapy. What’s more, 66% of those who received the new treatment were still alive at the end of the study period, compared with only 48% of those who received standard chemotherapy.The authors say side effects were similar for both groups, and serious adverse events were less likely for the sacituzumab tirumotecan group. The findings suggest that sacituzumab tirumotecan could be a more effective option than standard chemotherapy for people with hard-to-treat lung cancer driven by EGFR mutations.N. Engl. J. Med. 394, 13–26 (2026)Homing in on clones Tumours do not feature a uniform mix of mutated cells. Instead, they are made up of an assortment of related cell populations, or clones, shaped by two main types of DNA change. Some carry single-letter mutations, whereas others are characterized by the gain or loss of large segments of DNA. This complexity presents a challenge for clinicians and researchers trying to analyse tumour samples to understand the nature of a person’s disease and the best course of treatment.The standard approach for profiling tumours is bulk sequencing, which analyses DNA from many cells at once. But this method averages signals across millions of cells and so cannot determine which mutations occur in which clones, or disentangle overlapping genetic changes shared between them. Because cancer progression is driven by changes in individual cellular lineages, bulk sequencing’s lack of resolution limits efforts to reconstruct tumour evolution and to develop more-effective targeted therapies.To address this problem, Simone Zaccaria at University College London and his co-workers developed a method that uses patterns of single-letter mutations from multiple tumour samples to reconstruct when and in which cell populations large DNA gains and losses occurred. The authors report that this approach — called allele-specific phylogenetic analysis of copy-number alterations, or ALPACA — was able to detect hard-to-identify alterations present in a minority of the cancer cells in a sample.An analysis of tumours from a lung cancer study also revealed that the most aggressive clones had genomes that were significantly more unstable than those of other tumour cells. This suggests that genomic instability might help cancer cells acquire the ability to spread. Finally, the researchers showed that tumours with greater genetic diversity among their clones were associated with earlier relapse, which opens up the possibility of using this measure to predict patient outcomes.Nature 646, 190–197 (2025)
Five highlights from lung-cancer research
Treatment breakthroughs, improved screening approaches and other developments from recent studies.
1,476 words~7 min read