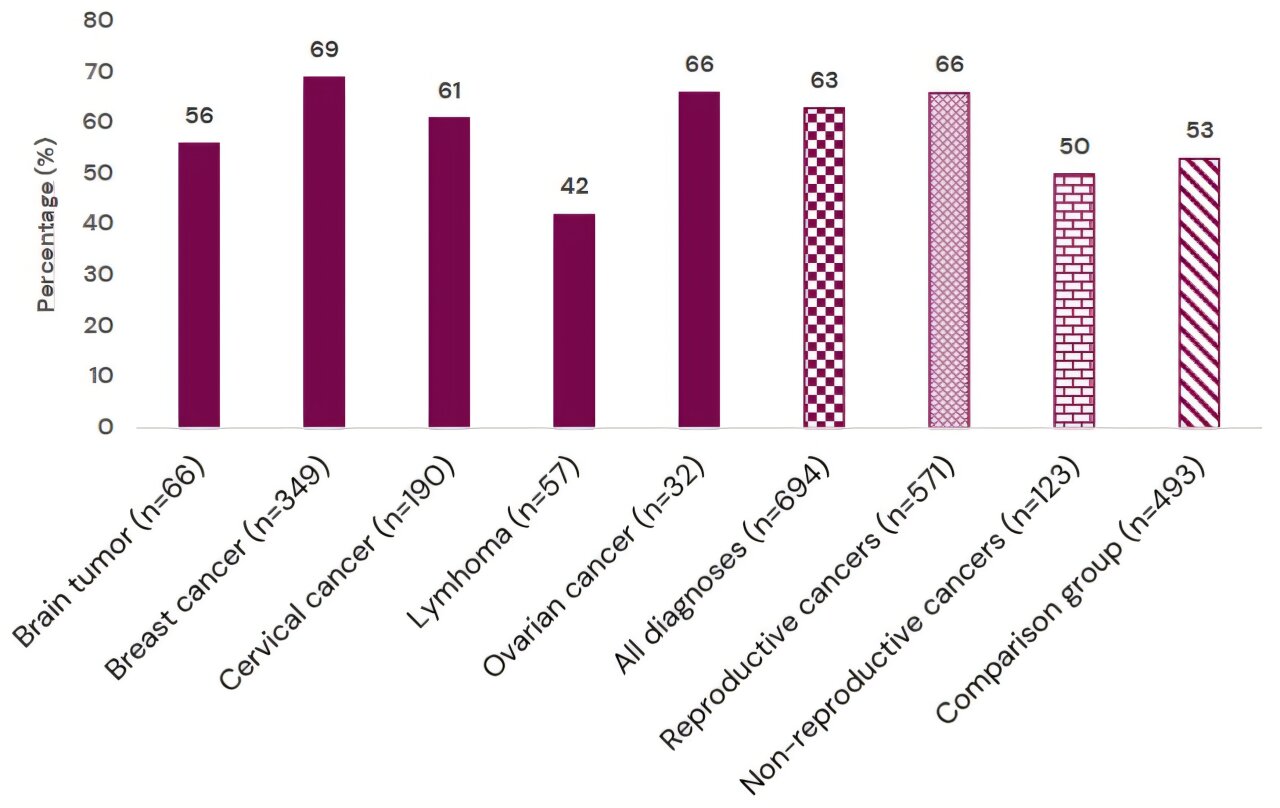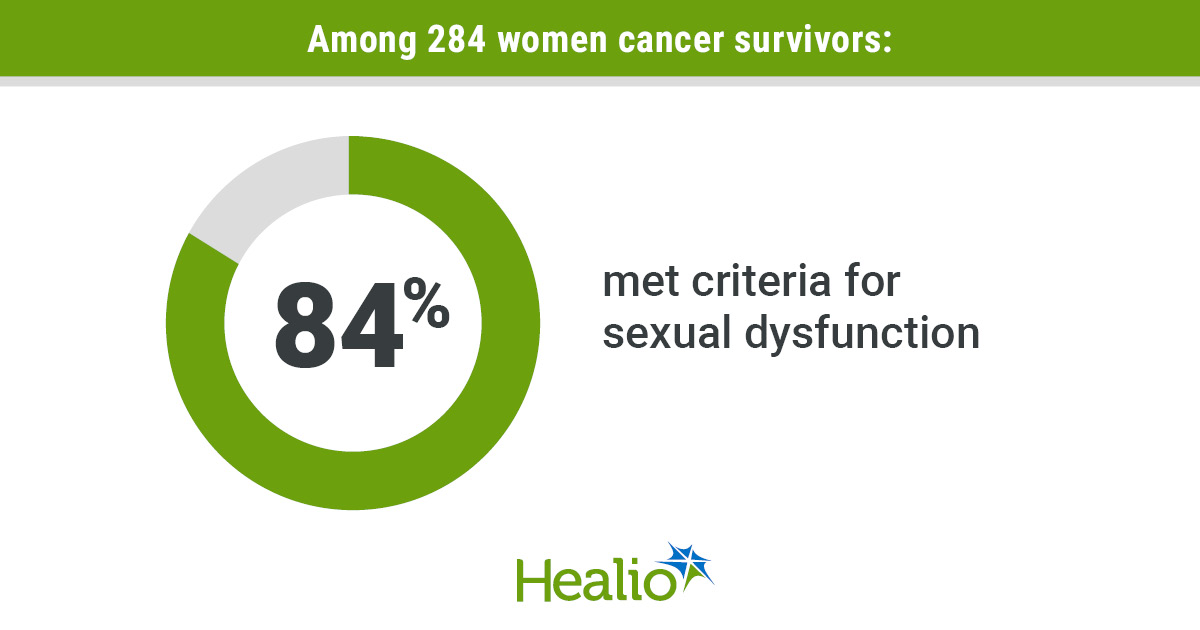
A new clinic at Davidoff Cancer Center helps patients and survivors rebuild intimacy after chemotherapy, surgery and trauma; doctors say sexuality is not a luxury, but part of recovery, identity and the will to liveSarit Rosenblum|The evening Eden and her partner were supposed to celebrate one year together became the most painful turning point of their lives. Instead of a restaurant table and a celebration of young love, they found themselves at an urgent care clinic facing a devastating diagnosis: Eden, 31, an artist and designer at the start of her career, had advanced cancer.The diagnosis came after five days of unusual fever and abdominal pain. “On the fifth day, I said, OK, instead of a restaurant, let’s go to urgent care,” Eden recalls. At the hospital, she was told she had stage 3-4 Hodgkin lymphoma. From that moment, she was forced to trade her paintbrushes for aggressive treatment cycles and a daily battle for her life.4 View gallery The impact of cancer on sexuality(Illustration: Or Yogev)The reality became even more complicated when the war broke out. A sense of physical insecurity and fear of being alone led the couple to move in together earlier than planned. Amid national and personal chaos, the intimate structure of their relationship underwent a painful transformation: her partner left his job, and the young romantic partnership gave way to a caregiver-patient dynamic.“I was completely crushed. I couldn’t get up from the couch by myself,” she says. “He declared himself my main caregiver and didn’t leave me for a moment. On one hand, that is amazing. On the other hand, the things that brought us close at the beginning of the relationship, sexuality and togetherness, disappeared completely. My illness put everything in a sensitive and unclear place.”As the intensive chemotherapy and biological treatments began, the physical space that had once been a source of pleasure became a source of fear. Blood thinners created an existential fear of injury or bleeding, turning intimacy into a potential threat. “They warned me that if I got injured, the bleeding wouldn’t stop. I knew that could also happen during sex, and I was very afraid,” she says.Extreme weakness left no room for desire. Eden describes trying to preserve fragments of closeness out of sensitivity to her partner’s needs, even as her own body betrayed her. “I gathered the strength to pleasure him, but slowly that also stopped. There was no possibility of pleasuring or being pleasured by anything connected to the body.”Months passed, and the disease receded. But the physical disconnect remained even after treatment ended and follow-up care began. The hope that everything would return to the way it had been was crushed into reality.A year and a half after her diagnosis, Eden is still mourning the loss of the ease and naturalness that once defined the relationship. Intimacy has turned from a source of comfort into a task requiring effort, practice and a constant fight against the body’s memory of pain.The trauma of treatment left her with extreme sensitivity that surfaces during moments of physical closeness. “Every little thing hurts,” she says. “During intimacy, pain suddenly surfaces in unexpected places, where it should not be felt. I tense up, and it ends right there.“To this day, we haven’t really returned to an intimate routine. From something that was simply fun, sex between us turned into exercises, difficulty, pain and anxiety. This takes work even when the instinct is to pull away. There is so much guilt and difficulty around it; it feels like yet another front in the battle. I often find myself grieving the fact that it hasn’t returned, and realizing I have to get to know myself all over again inside this new reality.”Cancer is not only a disease of the body. The psyche is also under attack. The first battle is, of course, for life. Against a sophisticated and elusive enemy, the first goal is survival in the most basic sense. But for many patients, the battle against the disease is not only a confrontation with cancer cells that have invaded the body. It is also a daily struggle over sexual identity and the couple relationship, an area often pushed aside because of medical urgency.Studies show that about 60% of women dealing with breast cancer experience significant damage to sexual function, including dryness, pain and a dramatic drop in desire following hormonal changes and treatment. Among men, the situation is similar: A Harvard University study of prostate cancer patients found that about 70% cope with erectile dysfunction following surgery or radiation.The difficulty is not only mechanical or physiological. Changes in the body and body image, including scars, hair loss or a feeling of betrayal and insecurity, create an emotional wall that makes openness and intimacy harder. When a partner becomes a caregiver instead of a lover, it becomes difficult to preserve the romantic spark.“I underwent a mastectomy and reconstruction because I wanted to regain a natural, feminine appearance. It was a long, complex operation, about 10 hours, followed by at least a month of recovery,” says a breast cancer survivor in her 40s.“Every evening, my husband changed the dressings and effectively became a nurse. The chest area and the abdomen, from which the tissue was taken for the reconstruction, looked terrible. He was really good at it, but the more grateful I felt for his devoted care, the more sexually distant I became. How can you feel desirable after your partner has seen you in that state?“Another disappointment came when I understood that as wonderful as the reconstruction looks, and as amazing as the doctors are, sensation in the breast will never return. An organ that was so warm and sensitive to touch became numb, a monument to what it once was. The love remained and even grew stronger, but you have to work on its physical expression. You have to find alternatives to what was familiar.”For Eyal, 43, “happily married” and a father of two whose career at El Al was at its peak, cancer was not only a biological invasion. It was a threat to everything that defined him as a man.Diagnosed with Hodgkin lymphoma at 37, Eyal had to confront the illness while also facing an old trauma. He lost his mother to cancer when he was 16, and the memory of her fighting to maintain a normal appearance was seared into him. “It was very important to her that people not know,” he recalls. “If someone knocked on the door, she immediately put on a wig.”When chemotherapy began to threaten his own appearance, old demons woke up. “There was enormous stress when the disease arrived,” says Eyal, a member of the “Stop Cancer” community for young cancer patients and survivors. “It connects to a lot of childhood insecurities, after years of self-work and understanding that I am a good-looking person and that my appearance is very important to me.“One of the side effects of chemotherapy is hair loss. Forget all the existential fears, suddenly you are also worried about losing a very significant marker of your appearance. Losing the look you are used to is a crisis. It sat in my head the whole time and sent me into a spiral: What will I look like? Will people accept me? Love me? Will I still look good?”The identity crisis peaked when his body began to change. “After the second treatment, I sat in the waiting room, put my hand on my head and when I lifted it, clumps of hair were left in my palm. That day I decided to shave it all off.”But the hair was only the beginning. Steroids and treatment changed the way his body felt, inside and out. During the long months of treatment, sexuality became an unattainable luxury. Eyal describes a state in which the body and mind shift into survival mode and libido simply disappears from consciousness.“It wasn’t on the table at all. At the beginning, doctors say, ‘These are unhealthy substances; you have to wait a few days before sexual contact.’ So from the start, you have to be careful. Later, you retain fluids from the steroids and feel completely swollen. The body is very sensitive, there is severe fatigue and you simply don’t feel sexual. The libido does not exist. You do not need sex. You cannot even imagine it.”For Eyal, as for Eden, the major crisis came precisely after the final treatment, when the medical envelope disappeared. “After six months or a year in which you are constantly surrounded and protected by doctors and tests, suddenly all at once you are left in a vacuum, with a mind that deals with the disease all the time: What if it comes back? Every small pain, every sensation, every sleepless night worries you because of the trauma. It took me a very long time to recover and accept my new body. I had to rebuild myself, to mend the breaks and wounds.”His return to himself was active and deliberate. He did not wait for the feelings to pass on their own, but set out on a rehabilitation journey that included intensive exercise and deep work as a couple. “I started training toward the end of the treatments. I wanted to return to a body I loved, one I felt comfortable with, not to be out of breath from every small action.”The attempt to restore what had been lost in the bedroom was accompanied by conflict and the need to learn the language of intimacy anew. “It took me a long time to let go, because when your head is preoccupied, things don’t work. "Physically, my wife adjusted to the new situation more quickly. That led to quite a few fights, because ultimately everyone wants to feel desired. But the body remembers. When the mind stops dealing with fear or anxiety about what might happen, it makes room for the body to work.“We sought advice and attended workshops to help rekindle it. It is work in every sense of the word. After 15 years, attraction is not the same as the raw passion of early dating, but you learn to make other things come alive: scent, touch, intellect. Slowly, you return to life.”One of the main barriers to coping with the loss of sexuality and desire during illness is the silence of the medical system. Caregivers do not often ask about the subject, and patients feel it is superficial or inappropriate to deal with sexuality when life itself is at stake.Studies published in the past have shown that patients feel the issue of sexuality rarely comes up in conversations with oncologists, leaving them isolated and guilty. Prof. Gal Markel, director of the Davidoff Comprehensive Cancer Center at Rabin Medical Center, points to a gap rooted in mutual embarrassment. “It is not only that patients don’t talk about it. Doctors don’t ask about it either,” he says.4 View gallery Prof. Gal Markel(Photo: Yuval Chen)According to Markel, while doctors tend to focus on physical side effects and clinical fears, patients are often troubled by existential questions about their identity. “Doctors think the patient is anxious about what side effects they will have or how much pain they will be in, when in fact much of what occupies them is entirely different questions, such as whether I will be able to keep working, function as a partner, as a parent, whether I will be able to continue providing, to be a friend, a family member. The effects on sexuality can come from countless directions, even if there is no direct injury to the target organs.”Treating sexuality among cancer patients, Markel says, is not a quality-of-life bonus, but a core part of modern medicine. “We are not treating a disease. We are treating human beings. Not only the patient, but also the family. I talk about this in every lecture I give. It is a significant part of our vision and mission.”How does that translate into practice?
Cancer took their sex lives; doctors are helping patients and couples find intimacy again
A new clinic at Davidoff Cancer Center helps patients and survivors rebuild intimacy after chemotherapy, surgery and trauma; doctors say sexuality is not a luxury, but part of recovery, identity and the will to live
3,855 words~18 min read