July 23rd, 2025
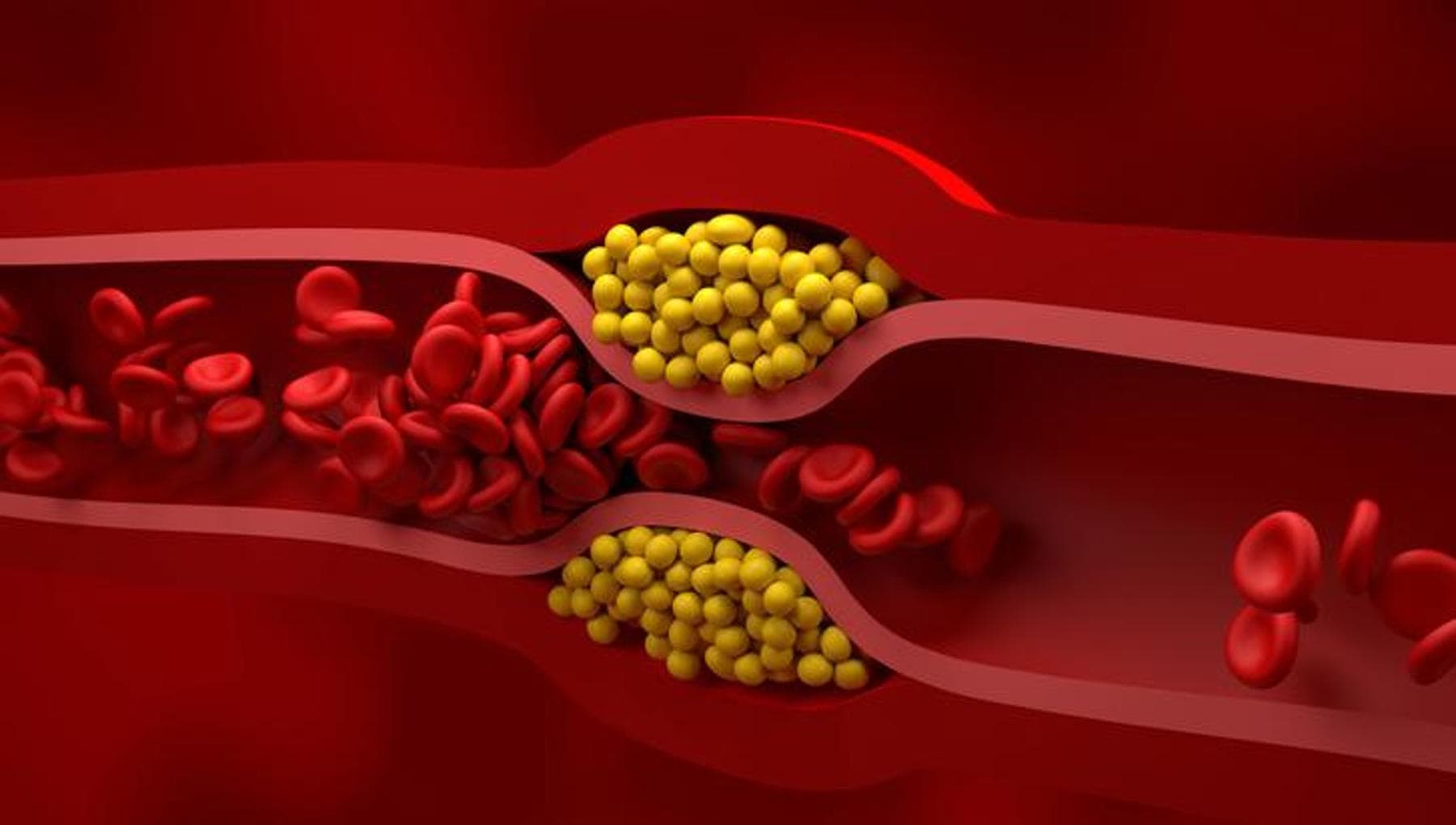
Most people who arrive an a hospital in the wake of a first heart attack or stroke due to rupture of an unstable atherosclerotic plaque in the arteries do not have elevated LDL cholesterol. This is cholesterol attached to LDL particles, coming from the liver for delivery to the rest of the body. While high LDL cholesterol is recognized as, on balance across a population, contributing to the pace at which plaque grows, it is not the whole story. It is probably not the most important part of the story either, given than the well-established therapies to lower LDL cholesterol do not reliably regress plaque, and only slow its growth somewhat.
Researchers have in recent years searched for and uncovered a broad range of other mechanisms that contribute to plaque growth in animal models of atherosclerosis. This has led to various markers, such as circulating Lp(a), that correlate with atherosclerotic plaque and consequent cardiovascular disease in human study populations. A number of biotech and pharmaceutical companies are working on the development of therapies to target these mechanisms, near all of which only produce a slowing of plaque growth when tested in animal models.