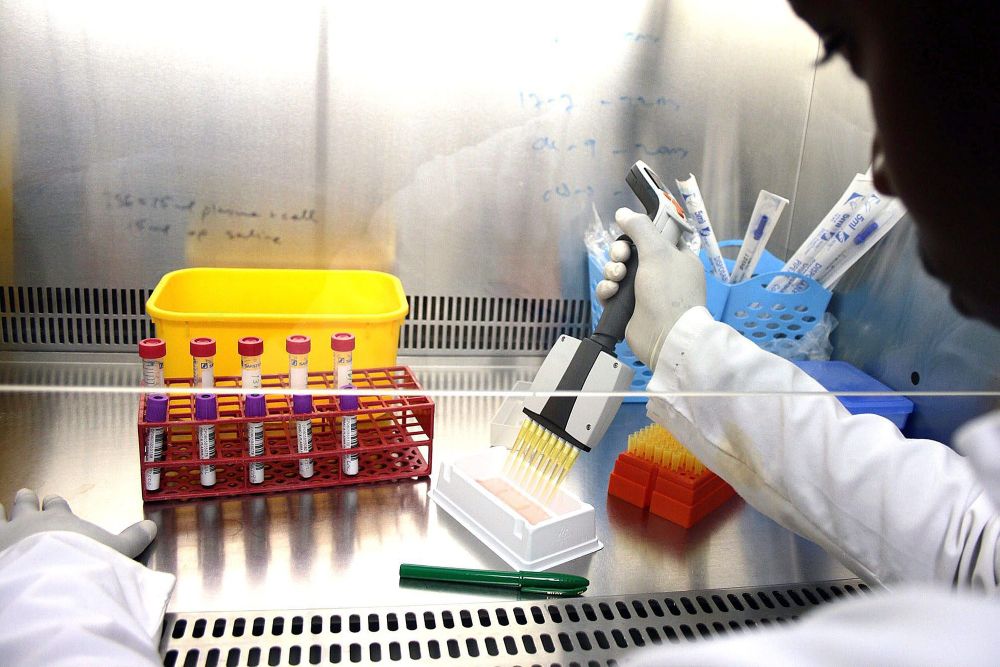
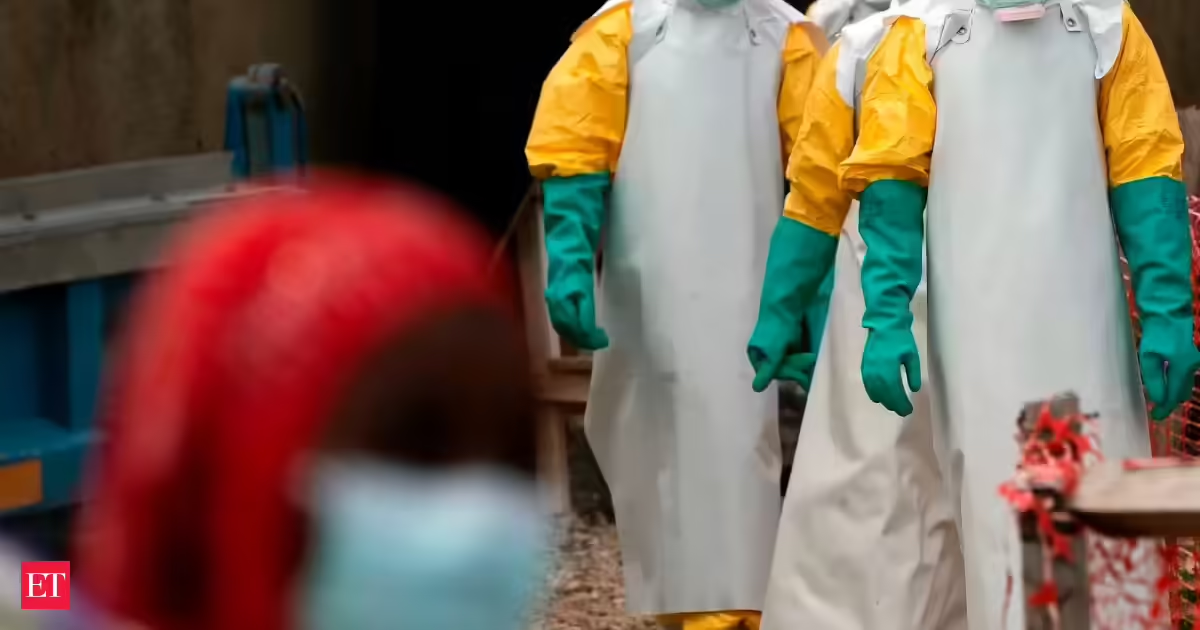
The current Ebola outbreak in the Democratic Republic of Congo (DRC) and Uganda is once again reminding the world that infectious diseases do not respect borders, visas, or geopolitics. In today’s interconnected world, an outbreak in Africa can become a public health concern for Asia within hours. That is precisely why India must respond with science, preparedness, surveillance, and calm leadership, certainly not fear, stigma, or panic.As of now, the outbreak involving the rare Bundibugyo strain (name derived from Bundibugyo district of Uganda in 2007) of Ebola has crossed alarming numbers. Reports suggest nearly 900-1,000 suspected cases in DRC, more than 100 confirmed infections, and over 200 suspected deaths. Uganda too has reported confirmed seven cases and one death linked to cross-border transmission. The World Health Organization (WHO) declared the outbreak a Public Health Emergency of International Concern (PHEIC) on May 16. The challenge is further compounded because this particular strain currently has no licensed vaccine or approved targeted antiviral treatment.India, fortunately, has not reported any confirmed Ebola case so far. That fact must be stated clearly and repeatedly. However, two recent suspected cases, one in Bengaluru involving a traveller from Uganda and another under observation in Gujarat, have naturally triggered concern and intensified surveillance measures across the country. Encouragingly, the Bengaluru case reportedly tested negative by PCR at the National Institute of Virology (NIV), Pune. A second PCR may be required to reconfirm.Let us understand this properly: suspicion is not confirmation. Public health systems are designed to isolate, investigate, test, and monitor suspected infections. That is exactly what authorities are doing. This is vigilance. This is preparedness. This is how responsible health systems function.Unfortunately, in the era of social media forwards and instant misinformation, even a suspected case can create disproportionate hysteria. We saw this during COVID-19 as also during Nipah and Zika scares. Panic spreads faster than pathogens.Ebola is undoubtedly a serious viral haemorrhagic disease with historically high fatality rates of 25% to 90%, but it is not casually airborne like flu or COVID-19. Transmission typically requires direct contact with infected bodily fluids, contaminated medical equipment, unsafe caregiving exposure, or certain burial practices. People do not catch Ebola merely by sharing airspace, sitting in the same room briefly, or casual day-to-day contact. Public understanding must be rooted in facts, not the WhatsApp mythology.Cautious approachIndia’s response so far has been appropriately cautious. Screening at airports has intensified. Isolation facilities have been activated in States such as Gujarat. SOPs have been issued for hospitals, laboratories, infection control, safe handling of suspected cases, and traveller monitoring. This reflects one of the most important lessons India learned during COVID-19: preparedness cannot start after community transmission begins.At the same time, India has demonstrated global responsibility by dispatching urgent medical assistance and Ebola relief supplies to Africa Centres of Disease Control and Prevention. This is not merely diplomacy; it is enlightened public health solidarity, which was also evident during ‘Vaccine Maitri’ during the pandemic. Infectious disease control anywhere helps protect populations everywhere. Global health security is built on solidarity, not isolation.What worries me most is not only the virus itself, but the larger systemic issues surrounding outbreaks. The current Ebola emergency is unfolding amid conflict zones, displacement, weak surveillance infrastructure, mistrust of authorities, and severe shortages of healthcare resources in affected African regions. Attacks on healthcare facilities in the DRC are severely hampering outbreak control efforts, with fear, insecurity, and mistrust even leading some suspected Ebola patients to flee treatment centres. Misinformation is making containment even more difficult. We must recognise that epidemics flourish where health systems are fragile and trust breaks down.Today, India is far better prepared than it was a decade ago. Our experience with HIV, H1N1, Nipah, COVID-19, Zika, Mpox (monkeypox), and other infectious threats has strengthened laboratory networks, surveillance systems, genomic monitoring, airport screening, PPE readiness, and rapid-response mechanisms. But preparedness is not a one-time achievement. It is a continuous process.The public also has responsibilities: do not spread rumours; do not stigmatise travellers or African nationals; do not circulate unverified videos or “miracle cures; do not fuel fear with misinformation or speculation.Instead, follow official advisories. Seek medical care if symptoms arise after travel to affected regions. Cooperate with surveillance and quarantine protocols if required. Trust evidence-based guidance.India should remain alert, but not alarmed.Public awareness must strengthen preparedness and not fuel fear. Science, surveillance, transparency, infection control, and public trust remain our strongest defences. Epidemics are prevented and controlled not by panic, but by preparedness and collective responsibility.Dr. Ishwar Gilada is a public health Expert and secretary-general, People’s Health Organisation-India. Views expressed are personal
On Ebola, India must stay alert, not alarmed
India must stay vigilant against Ebola, prioritizing science and preparedness over fear and misinformation during the ongoing outbreak.
763 words~3 min read