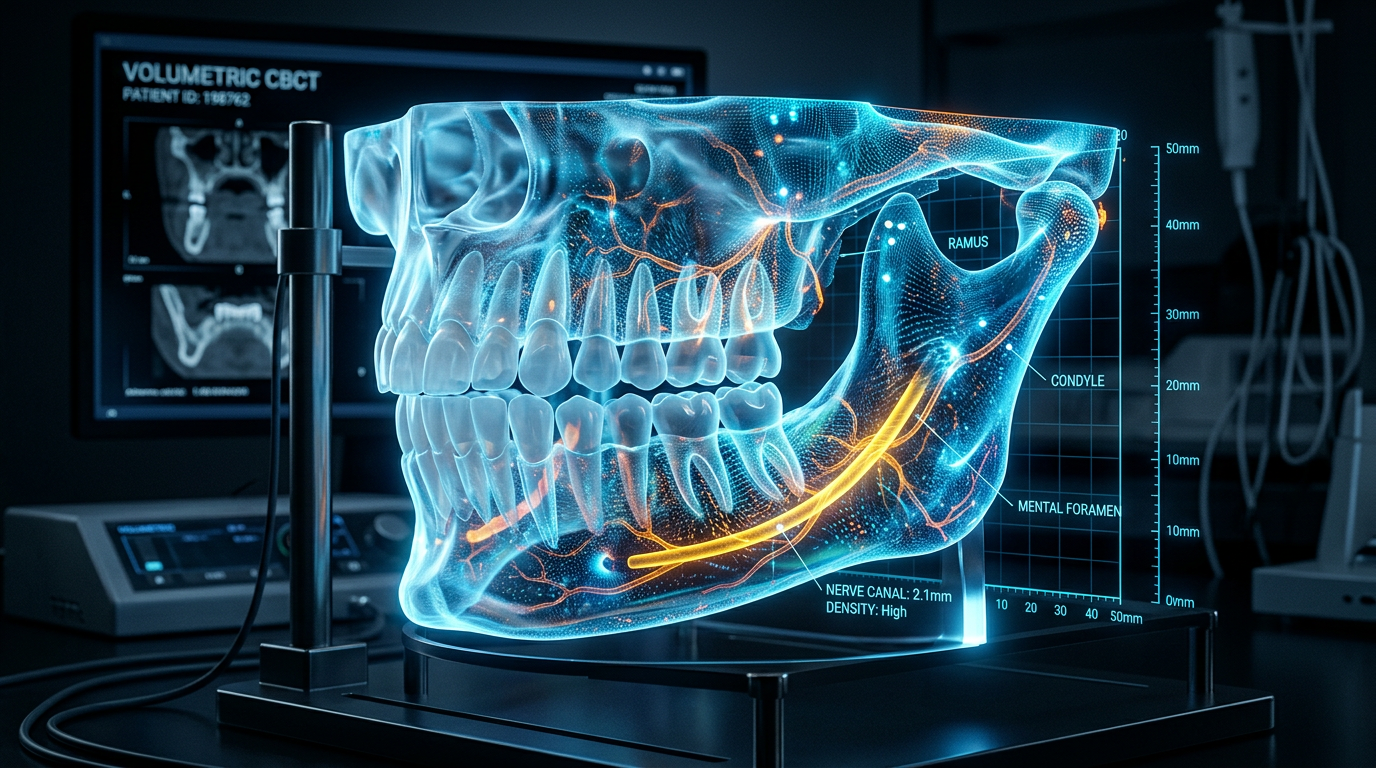
A detailed 3D volumetric CT scan of a human jaw highlights nerve pathways and bone structure
Most AI systems deployed in clinical settings today are assistive. They surface a recommendation, flag an anomaly, or highlight a region of interest in a scan. A human reviews the output and makes the call. The AI sits adjacent to the workflow rather than inside it.
What 21D has built in full-mouth dental implant rehabilitation is structurally different: an autonomous pipeline that handles the computational stages of surgical planning end-to-end, without a human planning technician in the loop. The system takes raw imaging data in, runs a sequence of AI-driven processing steps, and produces a 3D-printed surgical guide ready for the operating room. Approximately 98% of the workflow is automated. The surgeon’s role begins at the point of surgery, not before it.
Getting from assistive AI to autonomous AI in a surgical planning context required solving a specific set of technical problems that most clinical AI systems have not attempted. This article examines what those problems were and how 21D’s architecture addresses them.
The Core Technical Problem: Fragmentation Across Modalities and Systems