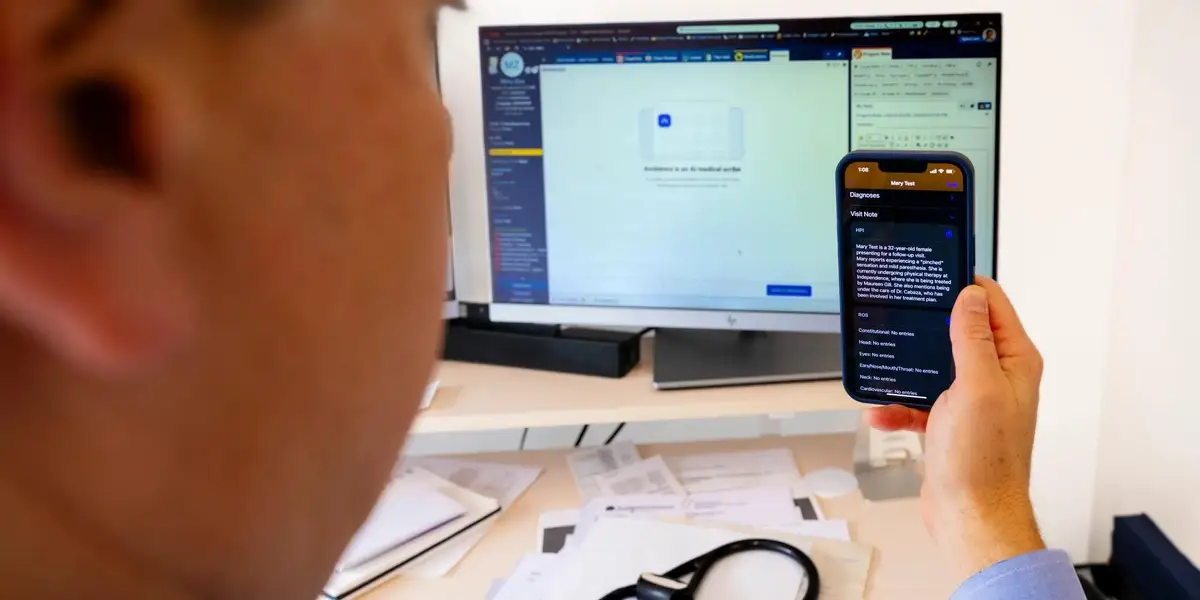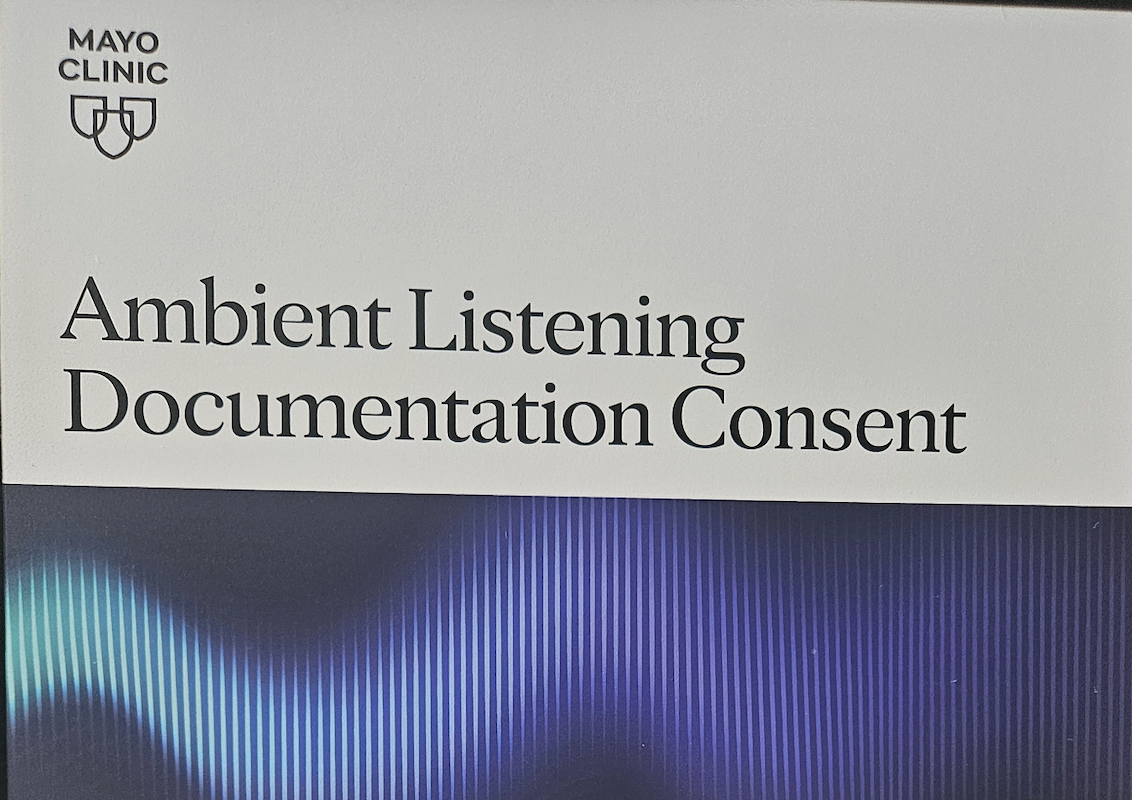
A patient completes a digital intake process at a healthcare facility. As healthcare documentation becomes more automated, questions about transparency and patient access to information are taking on new importance.gettyDuring a recent visit to a health system, I acknowledged that my clinical encounter would be recorded through an ambient AI application. A few minutes later, I walked into the exam room and saw a sign on the wall prohibiting “cell phone use, video recording or pictures” in the area.I realize there is some irony in taking a picture of a sign prohibiting pictures, but the contradiction was so explicit that I felt compelled to document it.The intake screen I had just completed read:“Indicates a required field.*Many providers are now using a new secure app that listens and drafts a note of your visit. If you prefer us not to use this technology, tell your provider at the start of your visit.*I acknowledge”“I acknowledge” was not a checkbox alongside multiple options. It was the only available action on the screen.I want to be very clear from the outset that I am not anti-AI. If anything, I am deeply optimistic about its role in healthcare. Earlier this year, I testified before the United States Senate about the importance of thoughtfully accelerating artificial intelligence across healthcare. My wife and I have also taken active roles in advocating for the safe, thoughtful and ethical deployment of medical AI because these systems are too important to deploy carelessly.MORE FOR YOUWhat struck me almost immediately about the intake language was the degree to which the interaction had already been framed before I arrived in the room. The system was not really asking whether I wanted to participate. It was informing me that this was already happening and instructing me to verbally interrupt the process later if I objected. Even the wording felt carefully constructed. The application “listens and drafts” a note, subtly implying that it does not “record” the encounter. Recording implies persistence, storage, replayability, ownership and discoverability. “Listens” sounds transient and almost passive, as though the interaction dissipates the moment the conversation ends.As someone who works in technology, my immediate reaction was essentially the mental equivalent of the SMH emoji. The language felt engineered to soften what was actually occurring. I could not even meaningfully consent. I could only acknowledge. As a patient, though, the experience felt less intellectual and more uncomfortable. I did not feel like I had a real choice.Patients enter healthcare environments from a fundamentally asymmetric position. They are dependent on expertise they do not possess, navigating systems they do not control, usually while anxious, exhausted, embarrassed, physically unwell or emotionally overwhelmed. Asking a patient to object verbally after the encounter has already started does not feel like casually selecting a different option on a form. It feels socially disruptive. It feels adversarial. It risks making someone feel difficult inside an interaction where they already hold less power than everyone around them.The sign on the wall made that asymmetry feel even more explicit. The institution was not merely declining to extend reciprocal recording rights to the patient. It was actively prohibiting them.Why this became very real for me emerged after one visit involving ambient documentation. I logged into my patient portal while attending a healthcare conference because I wanted to show someone what one of these generated notes looked like in practice. Instead, I discovered that my medical history now included “legal intervention involving injury by tear gas.” My surgical history also stated that I had undergone a complete revision knee replacement.I have never been tear gassed, and unless something happened without my knowledge, I still have my original knees.The tear gas entry was absurd enough that I laughed. The knee replacement entry unsettled me more because it represented the kind of error that could realistically propagate operationally through the healthcare system and influence future clinical decisions.What has now surprised me most is that I still have not corrected either one.Not because I do not understand healthcare operations, and not because I do not understand AI. I work directly in this space. I still do not fully understand the cleanest operational pathway for correcting the record, and I honestly have not had the time to navigate the process. Healthcare expects patients to catch inaccuracies, reconcile conflicting information and function as part of the system’s quality control process while simultaneously making it difficult to independently verify the underlying interaction itself.In one visit, a physician walked into the room with his phone face down on the counter already running in the background. He never mentioned it. I eventually asked because I was curious what the ambient scribe actually looked like operationally. In another visit, the physician at least had the screen facing upward where I could see the application functioning during the encounter, but again, nothing was verbally discussed. In both situations, the recording had effectively already begun before any meaningful conversation about participation had occurred.Patients receive not the encounter itself, but the system’s finalized interpretation of it after multiple layers of summarization and restructuring have already occurred.In radiology, the report does not replace the image itself. The underlying study still exists for clinicians and patients who want to independently review it or seek second opinions. Increasingly, ambient systems are creating a different dynamic around conversation itself. The interaction is captured, transformed, operationalized and returned primarily as interpretation.I am not arguing that every patient wants transcripts or recordings of their encounters. Many will not. I am also not arguing against ambient AI itself. I believe these technologies are going to become deeply embedded into healthcare delivery because the documentation burden facing clinicians is unsustainable. But I do believe patients should have access to the raw, uninterpreted interaction before AI summarization transforms it into a finalized narrative inside the medical record.Healthcare depends on patients to identify medication discrepancies, coordinate fragmented care, monitor follow-up, challenge inaccuracies and recognize when something inside the record does not align with reality. At the same time, the underlying interaction producing that record is increasingly being captured and controlled institutionally while patients remain downstream recipients of the finalized interpretation.The system says patients are partners. Partnership becomes difficult to define when one side controls the source material while the other is expected to identify failures inside a record they are not permitted to independently verify.
I Could Only Acknowledge
Ambient AI is transforming clinical documentation. But what happens when patients can audit the record, not the source?
1,053 words~5 min read