At least 12 of my colleagues boarded planes to the American Society of Clinical Oncology conference in Chicago last week to hear Charles Swanton of the Francis Crick Institute in London share results from the world’s first randomized trial on a multi-cancer early detection test.
The trial — a partnership between the U.K. National Health Service and Grail, which makes the Galleri MCED test — randomized 143,000 average English adults aged 50-77 to receive either usual care or MCED testing. The primary endpoint was reduction of stage 3 and 4 cancers across all cancer types.
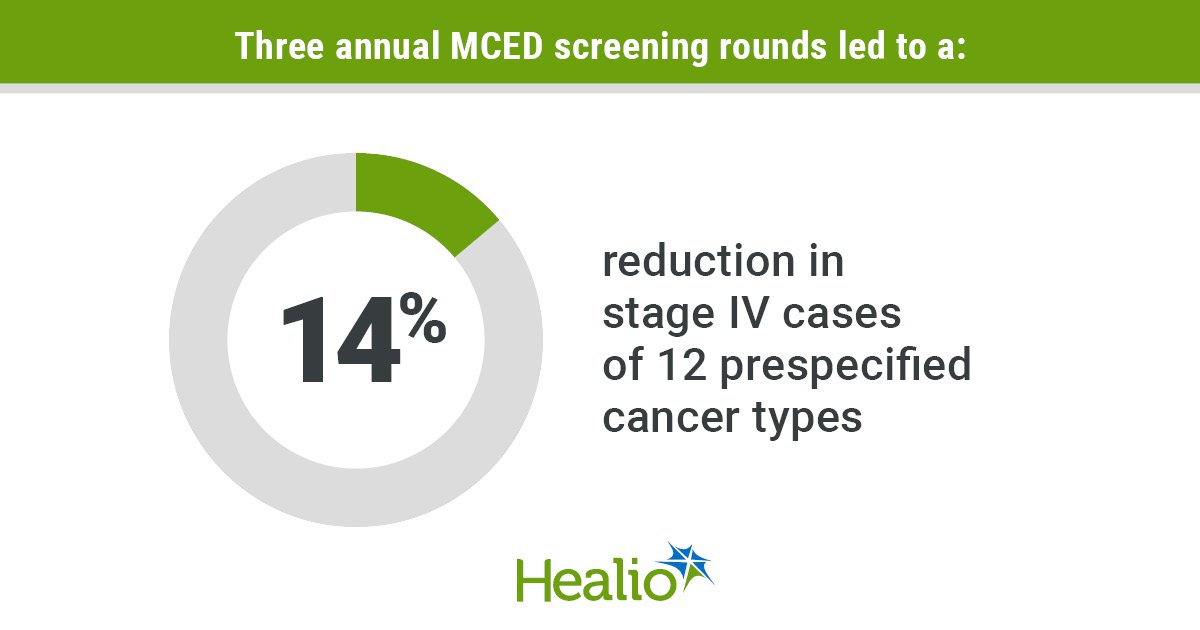
After three rounds of annual molecular screening, the trial failed to meet its primary endpoint — a punch line we have known for months. Nevertheless, hearing about the results in detail was invaluable.
As an oncologist and active researcher in the field of screening, I found a lot of promising signals in this trial. But technical and methodological challenges got in the way of clear results and definitive conclusions.
In 2025, the American Cancer Society published guidance for physicians on MCEDs. This January, a federal bill passed that enables Medicare to cover MCEDs if any are FDA approved, although no MCED is yet FDA approved or guideline-recommended, and the world of screening, primary care, and oncology has waited for evidence of clinical benefit for years. Understanding the statistical and epidemiological complexities that drove the negative results may help us get closer to assessing that benefit.