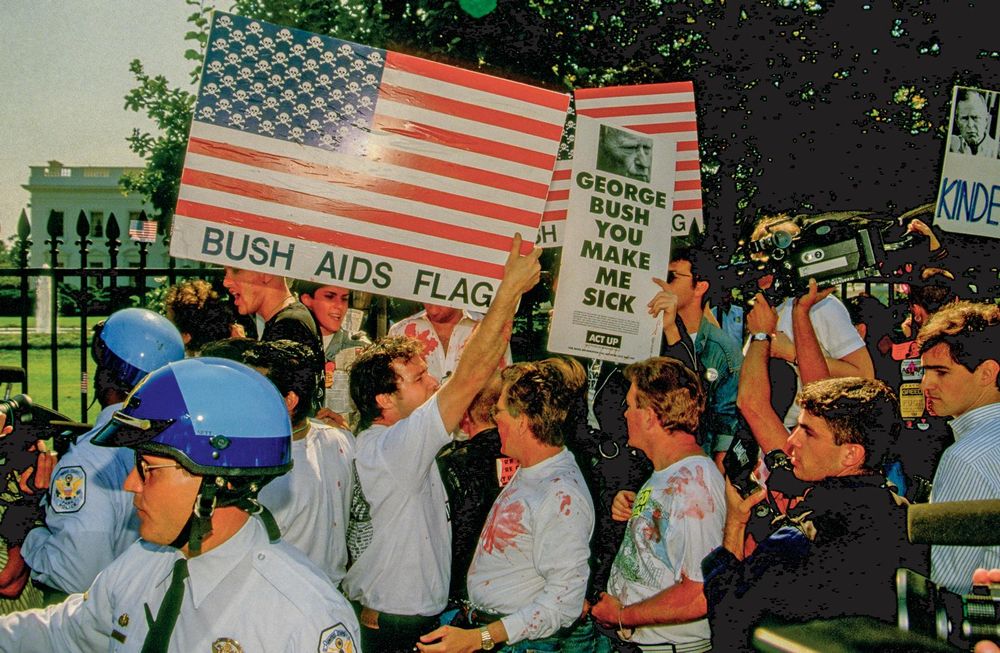
Shortly after 8pm on May 29th, 2023, my brother Brian, aged 62, died at London’s Whittington Hospital. He had been admitted by ambulance late the previous night following a collapse at a nursing home.At 11.40 that morning – observing his frailty – a doctor who did not know him advised against resuscitation should his heart stop. “We like to have this conversation earlier rather than later,” she wrote in her medical notes, “and given his complex medical history, he is unlikely to benefit from CPR and [it] is more likely to cause more harm than good.” At 7pm, with cannulas on each of Brian’s hands infusing dextrose and sodium, a nurse reported: “No concerns at present.” Less than an hour later my brother’s heart stopped. By the time his stillness was noticed, he was no longer breathing. There was no resuscitation. “On review, indeed, no signs of life.”His partner was contacted.“Title of conversation – condolences.”“Mode of conversation – telephone.”Brian’s death certificate recorded the immediate causes of death; a pneumonia caused by food and liquid entering his lungs – and a “pseudo” internal obstruction.The underlying causes were: human immunodeficiency virus, the cancer Kaposi’s sarcoma (KS) and severe frailty.By the time he died, Brian weighed just over eight stone, having lost four stone “unintentionally” in six months. He had cachexia, wasting syndrome, his clothes loose around his body.The russet lesions of KS – a cancer consigned in public memory to last-century deaths from Aids yet still recorded by the World Health Organisation as “Aids defining” – were visible on his legs, arms and chest.Everything about this death – the virus, the cancer, the wasting – felt as though from another time.Emily O’Reilly: 'After his death, my conscious self split in two.' Photo: Bryan O’Brien/The Irish Times Brian had died more than 40 years after the western Aids epidemic began, more than 30 since his HIV diagnosis, a quarter of a century since effective HIV treatment had emerged. Why then, at the end, did he look less like a survivor of the modern HIV era than a casualty of its first?After his death, my conscious self split in two. One part was a grieving sister, mourning the loss of a brother, friend, confidant, beloved of my children, his Christening my first conscious memory.Emily and Brian O'Reilly on the day of his Christening The other part was the curious professional – a former journalist, Ombudsman – wondering at the disconnect between the contemporary framing of HIV and my brother’s final two years and death.His dying seemed impolite, offending against the narrative: that, with treatment, the crisis had passed, that people would live lives as long as anyone else’s.But if that were true, how could someone whose HIV was well controlled by antiretroviral therapy die like this – in London – in 2023?How was it possible for someone to get KS on the very treatment that is meant to hold it in check? And if that cancer is – still – categorised as “Aids defining” – what did that mean in his singular case?In a scant two years, Brian’s body had unravelled, developing cardiac, renal and liver failure alongside electrolyte instability that caused blackouts. A sling supported a shoulder fractured and repaired after a fall. Nerve damage to a foot confined him to a wheelchair. Chemotherapy in late 2022 weakened him; his body still dealing with the aftermath of intestinal surgery six years earlier, albeit successful.I keep our final WhatsApp: ‘You about?’ he wrote, ‘Yup,’ I repliedTwo nights before he died, we spoke for the last time, about family, relationships, from his plans for a move to a new nursing home later that week, to a pint in a Kensington pub in a wheelchair gifted by a friend.I keep our final WhatsApp. “You about?” he wrote. “Yup,” I replied. Brian had emigrated to New York in 1982, aged 21, away from his family, from his architectural studies, away from an Ireland mired in a homophobia so normalised that the gap between the official criminalisation of gay male sex and the unofficial violence against gay males was at times paper thin.In September of that year, five teenage boys beat to death 31-year-old Declan Flynn with branches wrenched from the birch trees of Dublin’s Fairview Park.One of his killers – aged 14 – described the act as “queer-bashing”. Brian O'Reilly pictured in his 20s. He emigrated to New York in 1982. In 1990 he tested positive for HIV The judge suspended their manslaughter convictions, commenting: “One thing that has come to my mind is that there is no element of correction that is required. All of you come from good homes and experienced care and affection.”As Brian planned his New York life – arriving at a peak of sexual freedom for gay men – a new threat was quietly announcing itself.A June 1981 report from the Centres for Disease Control and Prevention described a rare lung infection, pneumocystis carinii pneumonia, in five gay men in Los Angeles. Two had died.It was the first official report of what later became known as Aids. By 1995, one gay man in nine in the US had been diagnosed with Aids; one in 15 had died.In 1990, Brian tested positive for HIV. Briefly returning to Ireland, he moved to London, remaining there with his partner for the rest of his life. [ Hundreds gather in Dublin to remember Declan Flynn 40 years after his deathOpens in new window ]In 1997, the roll out of new antiretroviral drug regimens dramatically increased life expectancy. The terrors passed. He would live, but in a space that demanded vigilance, monitoring, blood checks, medication changes as side effects emerged – high cholesterol, anxiety, potential cardiac and kidney risks – 15 different antiretroviral therapy regimens between 1997 and 2022.All of this – to me – was invisible. His chemical sentinels demanded attention, yet remained in the conversational shadows.By the turn of the century, the HIV/Aids story was shifting. Online Aids memorials were less frequently updated; the remembered dead eternally stuck in the gay style subcultures of the decades they had died in.HIV was there just as diabetes was or any chronic disease. Fewer people remembered the epidemic, even fewer its iconic disease – KS.I trace the start of my brother’s decline to Easter 2021. It came early that year. We met in London in late March. Walking down Euston Road, he was limping, his left foot dragging. En route to Sainsburys one day, he tripped. Passersby plucked him from the hedge he had tumbled into.By the following summer he required a leg brace, ultimately, a wheelchair. An abnormal heart rhythm emerged in May; an attempted surgical fix failed two months later. His chemical sentinels demanded attention, yet remained in the conversational shadowsIn September, his kidney function deteriorated.His sodium levels fluctuated. He would faint, have seizures, attend A&E departments for sodium infusions.Brian coped, using a spreadsheet to monitor test results, track appointments, forward emails, corral his siloed consultants. I hovered as he shared the latest, speculative, diagnoses of his doctors; spinal cancer, breast cancer, motor neuron disease. In March 2022, an older, more terrifying world returned. Lesions on his knee and ankle had concerned his GP, a biopsy to check for KS was planned. His HIV consultant said KS was “highly unlikely”. The markers of his immune defence were normal, his viral load undetectable. Days later, a biopsy confirmed the cancer.He had options. This form of KS might remain on the skin and not spread into organs. He could die with it, and not because of it.Brian did not want it, period. He craved chemotherapy, terrified of facial lesions. In a hospital day room one morning, he watched as people received intravenous chemotherapy.I envied them, he said. My brother was not a child of the 21st century with its optimistic HIV narrative, with Aids at least tamed – not even called Aids any more – but rather “advanced HIV” and everyone expected to live long and healthy lives.Brian was a child of the 1980s western Aids epidemic, when tens of thousands of gay men died and the lesions of KS did more than signal illness. They marked you.Four rounds of chemotherapy later, bruised from another fall, his treatment was stopped. Some lesions had faded; fresh ones arose on his legs, arms and chest. The spring of 2023 brought more weight loss, more falls, a medication list so long, that in itself – “polypharmacy” – carried the weight of a separate illness.I looked for answers to his death, to those final, brutal, two years, to the inability of myriad specialists to identify a unifying ‘why’ or to keep him aliveA shoulder break required an operation and physiotherapy that he was too weak to endure.He took vitamins, painkillers. He carried from hospital to home and later to care home a plastic bag filled with liquid food supplements. Medical notes suggested that he swap strawberry flavour for chocolate. Brian had worked for a global corporation. In 2022, no longer able to do so, he lost his job and his health insurance, moving from private rooms, bespoke menus and – in one hospital – views of the playing fields of Harrow – to the chaos of overcrowded NHS wards and finally to a nursing home from where he was brought, on an early summer’s night, to Whittington Hospital to die.Eight days after his death, the nursing home, in an email, attached its condolences to an unpaid bill.Following his funeral in London, my brother, sister and I – a cat’s cradle of hands beneath the casket – placed his ashes in our parents’ grave.I looked for answers to his death, to those final, brutal, two years, to the inability of myriad specialists to identify a unifying “why” or to keep him alive.I searched for a missed diagnosis, an overlooked infection, a hidden cancer that might explain the catastrophic failing of his body. [ Aoife was diagnosed with HIV in Australia in 2020: ‘He was unknowingly positive. We had no idea’Opens in new window ]As administrator of his estate, I had access to his medical records.Thousands of pages – unredacted – landed in my inbox. Over months, I studied them, rabbit holes of detail charting the minutest of procedures; the raising of a bed rail, the administration of a single tablet, the subdivision of a daily calorie intake. Occasionally, one could sense someone standing back, observing this cascade of illnesses, marvelling at their profusion, musing about HIV, the possible spread of KS, inter-organ damage, undetected other cancers, one medication interfering with another, the notes littered with upside down question marks, the medical shorthand of perplexity.His emotional state was noted. “Patient visibly anxious”, “frightened”. Emily O'Reilly pictured in her office in September 2013 as she published her final report before taking up the role of European Ombudsman at the European Parliament in Strasbourg. Photograph: Bryan O'Brien/The Irish Times Obtaining his HIV clinic notes continued to prove difficult, the illness still carrying layers of privacy and protection and shame.I met his HIV consultant. He asked if a student could attend as he, the student, “hasn’t done one of these before”. The student – younger than my son – was already in the room, my dead brother and I now a teaching moment.A “constellation of medical problems” had led to Brian’s decline and death, the consultant said. His deterioration was very apparent, but it was “hard to label him as terminally unwell”. The emergence of KS was an “unexpected and very unusual scenario” for someone undetectable with a good CD4 count – a key indicator of immune system health – for so long. The terms ‘accelerated ageing’ and ‘accentuated ageing’ recurred across the literature, with calls for the greater integration of the science of biological ageing with HIV careListing Brian’s illnesses, he said none were linked to HIV, concluding that while HIV and KS were “mentioned” on his death certificate, they had not been “major players”. I understood the clinical distinction; HIV did not directly cause Brian’s cardiac, kidney and other system failures as once it had caused normally quiescent infections to run amok, yet the attempt to detach Brian’s death from the virus he had lived with for 33 years, jarred.I turned to medical literature, using search terms that might give coherence to medical incoherence. What emerged was something less tidy, less clear cut, the possibility that there was no single explanation at all.Paper after paper described “premature frailty”, “multi-system illness”, “wasting”, “polypharmacy”, the earlier onset of diseases associated with ageing despite effective HIV treatment.Brian ticked every box. His consultant had told me, “… ageing in people who have had HIV for a long time is an emerging topic that we are still learning about”.[ Irish rate of HIV diagnoses highest in western EuropeOpens in new window ]A lot of people, it appeared, were doing so. In 2021, as Brian’s illnesses began to gather, The Lancet medical journal – in the first of a series of papers on ageing with HIV – had noted that prolonged survival with HIV translates – even on antiretroviral therapy – into an “increase of non-Aids-defining illnesses associated with age”.The terms “accelerated ageing” and “accentuated ageing” recurred across the literature, with calls for the greater integration of the science of biological ageing with HIV care.What had happened to Brian was hiding in plain sight; his biological clock appeared to have detached from his chronological age. The old epidemic had changed tempo but Brian’s generation of people with HIV had had to age before science could see that, to see clinically what ageing with HIV looked like. It was one thing to examine cells under a microscope, another to see a hypothesis played out in a human being many years later.Brian’s generation had lived through the uncontrolled first encounter with the virus, through successive generations of treatment, surviving into middle age many years after the epidemic’s peak.The treatments extended life dramatically, but many early regimens carried toxicities that became fully visible only over time.[ Continued rise in HIV diagnoses after drop during pandemicOpens in new window ]HIV had not produced the catastrophic immune collapse associated with the epidemic years, but decades of immune activation, illness and treatment perhaps exacted a slower, cumulative, price.The role of KS in Brian’s death remains unresolved. It did not appear to be the aggressive KS of the epidemic years but nor did it appear to be the slower moving “classic” KS. Nothing else had been found to explain the wasting that had consumed him.No one said, “this is what he needs to get better”. Interventions were reactive, fragmented: sodium levels corrected, falls treated, scans ordered. Each intervention made individual sense, collectively they mirrored the dissonance of his decline.My brother has now been dead for three years. I have found no simple answer to the question I had asked then: how do you die like that when the dominant post-crisis consensus suggests that people on effective HIV treatment are no longer expected to die this way?What I found instead is that ageing with long-term HIV can look like this for some of the first western epidemic generation: not one catastrophic opportunistic infection, not the old Aids deaths of the 1980s and 1990s, but rather an accumulation of frailty, inflammation, malignancy, organ damage, medication, fear and exhaustion.My brother’s story had not been drawn from an older playbook. It was not out of date, not an outlier, not drawn from an obsolete HIV past.It was, rather, recognisably contemporary.Emily O’Reilly is a former European and Irish Ombudsman and journalist, currently serving as an Ambassador for the Open Government Partnership.
Emily O’Reilly: My brother’s HIV seemed under control. So why did he die?
Brian had lived through the 1980s epidemic; the 21st century HIV narrative was optimistic, with Aids tamed and everyone expected to live long and healthy lives
2,598 words~12 min read