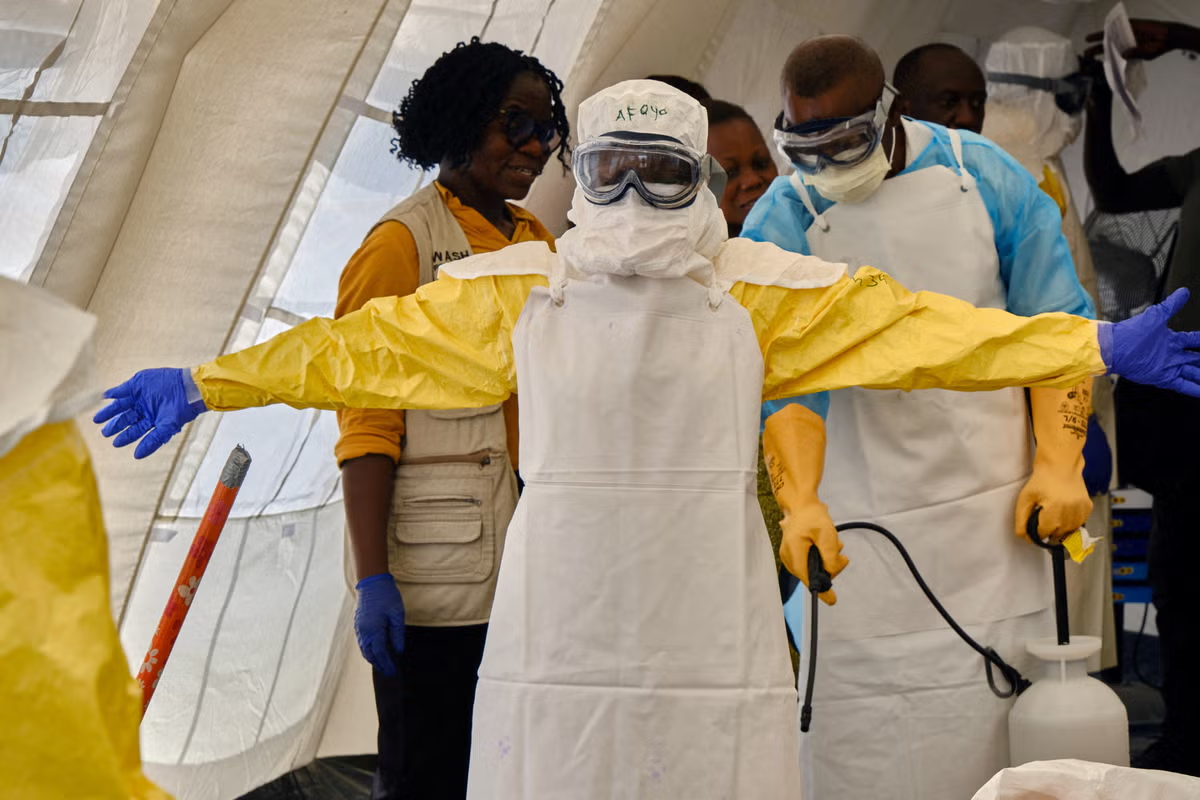
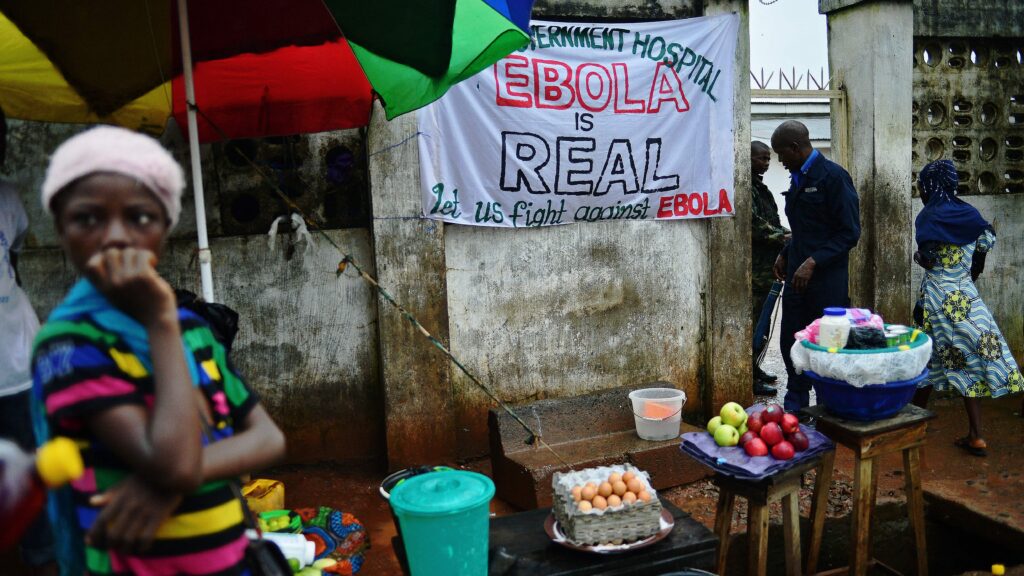
When I worked the Ebola outbreak in the South Kivu region of the Democratic Republic of Congo (DRC), the virus was not the only thing attacking people. An incredible amount of violence was also directed at the people who had come to stop it. Health workers were threatened. Some were killed. Treatment centres in the eastern provinces were burnt to the ground. The reflex, from a distance, is to call this irrational. It was not.Consider what people actually saw. Teams arrived in Tyvek suits that made them look extraterrestrial. They took family members into Ebola treatment units and about half of those who went in did not come out. People concluded that these outsiders had not come to save their community but to erase it. That conclusion was wrong. It was also reasonable, given the evidence in front of them. There was no trust, because the system had not earned it.I have come to believe that distrust is rarely ignorance. It is usually memory.That reframing matters, because we keep making the same diagnostic error. We treat distrust as a deficit of information, something to be corrected with a better pamphlet or a clearer graphic. So we send more messaging and we are surprised when it changes nothing. The people refusing our help are not missing the facts. They are recalling a different set of facts, drawn from their own experience, and reaching a defensible conclusion about institutions that have not been trustworthy to them.We saw the same mechanism at play during the Covid-19 pandemic in the US. The pattern of vaccine hesitancy was surprising to many. Black communities and registered Republicans, regardless of race, had the highest rates of hesitancy. Those two groups share little politically. What they do share is a history of reasons to doubt the institutions doing the asking. Different memories, same logic. People withhold trust from systems that have not been trustworthy to them and they are not wrong to notice.This is not a problem that messaging solves, because it was never a messaging problem. It is a structural one. Trust is not a mood. It is infrastructure. It is built the way any infrastructure is built, slowly and locally, by people who are present before the emergency and who remain after it ends.I have seen what that infrastructure looks like when it exists. In South Africa, I worked alongside community health workers who carried HIV medications into rural areas that the formal system could not reach. They succeeded for one reason: they were trusted, because they were of the community, not parachuted into it. They had standing that no clinic and no government carried. In the US, community health workers do the same work and hold the same trust, particularly in places where people have long and rational reasons to distrust the government. Yet here we have built almost no mechanism to pay them. In our system, if you cannot bill for it, it does not exist. So we have largely excluded the one workforce best positioned to close the gap, in precisely the communities where the gap is widest.There is a temptation to read the DRC and the US as separate stories, one about a fragile state far away and one about our own polarised politics. But they are the same story. In both, distrust tracks with lived experience. In both, the responses lean on outsiders in protective gear and official assurances, and in both, that response has limited credibility with the people who need the resources. The virus exploited the distance between institutions and communities, because that distance is where transmission lives.The work, then, is not to lecture communities into trusting us. It is to become trustworthy, which is slower and less satisfying and cannot be done in the middle of an outbreak for the first time. It means investing in the people who already hold the trust, paying them, and embedding them in the system rather than treating them as charity. It means recognising that public health does not happen to a community. It happens with one, or it does not happen at all.We must depoliticise public health. But before that, we have to earn the right to be believed.• Tyler B Evans is the founder and CEO of Wellness Equity Alliance and the author of ‘Decoding the Social and Political Drivers of Pandemics from Plague to Covid-19’. He served as the first chief medical officer for New York City, overseeing its Covid-19 response, and has worked in global health across dozens of countries for nearly three decades, including the two largest recorded Ebola outbreaks yet — 2015 in Sierra Leone and 2019 in the DRC.
TYLER B EVANS | From Congo to America, distrust in public health reads the same way
Ebola outbreak and vaccine hesitancy show institutional betrayal breeds distrust
774 words~4 min read