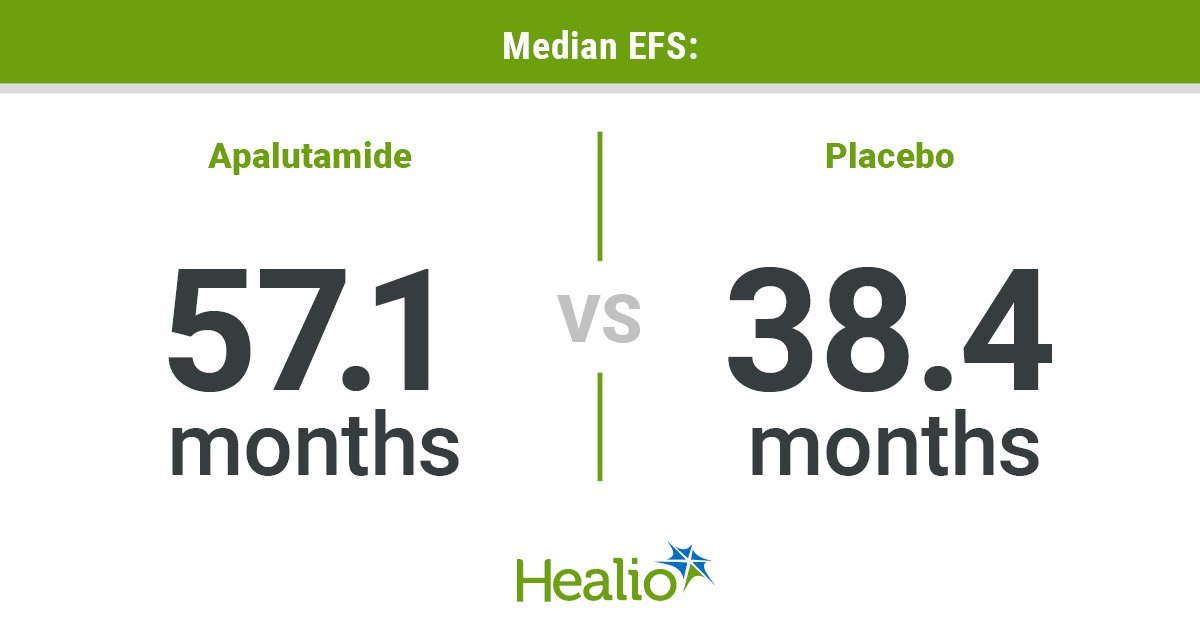
A new regimen involving Johnson & Johnson’s prostate cancer drug Erleada, when combined with hormone-blocking therapy, has shown significant promise in improving outcomes for patients undergoing prostate surgery. Data from a late-stage trial, presented on Sunday, indicate that the treatment, administered six months before and after surgery, substantially increased the chances of eliminating cancer and reduced the risk of disease progression or death.The study, which tracked patients for over five years, revealed that individuals receiving this combined therapy were nine times more likely to have minimal to no detectable cancer in the prostate at the time of surgery, compared to those who received testosterone-blocking therapy alone. Johnson & Johnson's prostate cancer drug Erleada, used with hormone-blocking therapy six months before and after prostate surgery, improved the chances of eliminating the cancer (Getty Images)Furthermore, the addition of Erleada reduced the risk of cancer spreading or causing death by 20%, according to the company.These findings, unveiled at the American Society of Clinical Oncology meeting in Chicago, are expected to reshape how doctors approach the treatment of men diagnosed with high-risk localized or locally advanced prostate cancer. Currently, the standard of care for such patients typically involves surgery to remove the prostate and radiation therapy.Johnson & Johnson noted that approximately 40% of the 330,000 individuals diagnosed with prostate cancer in the U.S. are classified as high-risk.About 40% of the 330,000 people diagnosed with prostate cancer in the U.S. are considered high-risk (Alamy/PA)The trial also investigated a full year of Erleada and hormone therapy before and after surgery. In this group, men on the combination therapy went, on average, more than six years before requiring subsequent treatment, nearly doubling the time observed for those on hormone therapy alone. This extended Erleada therapy also reduced the risk of recurrence and death by 29%.Nearly half of patients who undergo the current standard prostate-removal surgery and radiation experience a return of their cancer, necessitating additional treatment, J&J stated."No ARPIs are approved for localized high-risk prostate cancer with either surgery or radiation. So the (data) would be paradigm-changing," said Dr. Mary-Ellen Taplin, the study's lead researcher from Dana-Farber Cancer Institute in Boston.Erleada, chemically known as apalutamide, is an androgen receptor pathway inhibitor, a class of drugs that blocks signals driving prostate-cancer growth. The trial enrolled over 2,000 patients with high-risk localized or locally advanced prostate cancer who were candidates for prostate gland removal surgery.At the time of surgery, 8.9% of patients on the combination treatment had little to no detectable cancer, a stark contrast to 1% of those receiving hormone therapy alone."The patient benefit here is unequivocal," Mark Wildgust, J&J's medical affairs lead for oncology, said in an interview. "I think that the evidence is really showing that Erleada is adding something that we had not seen before."Other widely used ARPIs include Pfizer's Xtandi and Bayer's Nubeqa.J&J confirmed that the safety profile of the Erleada combination treatment was consistent with previous studies. Common side effects reported among patients included hot flushes, urinary incontinence, and erectile dysfunction.Erleada received U.S. approval in 2018 and is currently used in conjunction with hormone therapy that suppresses testosterone production, a key driver of prostate cancer growth. The company plans to collaborate with regulators to secure global approval for this combination therapy in earlier stages of prostate cancer.
Prostate cancer breakthrough as drug combo gives patients a powerful new chance
Data from a late-stage trial, presented on Sunday, indicate that the treatment, administered six months before and after surgery, substantially increased the chances of eliminating cancer and reduced the risk of disease progression or death
544 words~2 min read