TEMPO.CO, Jakarta - A new Ebola outbreak is circulating in the Democratic Republic of Congo. Genetic evidence suggests it had been spreading for weeks, possibly months, before it was detected. The strain is current, and much about its specific behavior remains unknown, according to DW.Understanding why the virus spreads as it does begins with how it enters the body. Unlike respiratory viruses that travel through air, Ebola requires direct contact.How Ebola virus enters the bodyThe virus enters through mucous membranes in the mouth, nose, or eyes, or through cuts and wounds in the skin. Intact skin acts as a barrier, but any break becomes an entry point.David Heymann, an epidemiologist at the London School of Hygiene and Tropical Medicine who first studied Ebola in 1976, describes transmission in practical terms:"The Ebola virus is spread from person to person by body fluids. So that means by blood, by saliva, possibly by feces, by urine, and also we now know in persons who are recovered through the semen."The virus relies on these routes because they provide direct access into the body.Infected people shed large amounts of virus in these fluids.Healthcare workers handling bodily secretions without protection face particular risk.Family members caring for patients in late-stage illness, when viral load is highest, are also highly exposed.What happens inside: a systemic attackThe virus does not attack randomly.Bodo Plachter, professor of virology at the University of Mainz in Germany, explains the mechanism:"The virus will always replicate at the site of entry in the lymph nodes, but then it spreads throughout the body and gets carried away by cells through the bloodstream to different organs."Crucially, it first targets immune cells — the body’s own defenders. Once these are disabled, the immune system cannot respond effectively.The result is severe systemic infection, with extremely high levels of virus in bodily fluids, increasing the risk of transmission for caregivers and medical staff.Symptoms: how the disease progressesHeymann, who has observed Ebola clinically and epidemiologically for decades, describes a disease that can initially resemble common infections."The initial signs and symptoms are like any other minor disease, like a cold, an infection, even like malaria. Then, in some instances, people begin to feel better. After that, they then begin with a hemorrhagic disease where blood begins to ooze out from different body orifices."That apparent improvement can be misleading. By the time the disease becomes clearly identifiable, patients are often at peak infectiousness."The people who are most infectious are the people who have the most virus in the solution or the body fluid that infects. So, if there's blood contamination of a person who's dealing with a patient, that will be full of virus,” he says.This timing creates a critical risk window for healthcare workers and family members.Why Ebola remains infectious after deathDeath does not immediately eliminate the virus. Bodies of people who die from Ebola can still contain high levels of viable virus in blood, tissue fluids, and other secretions.Heymann explains:"There's a ritual of cleaning the body and doing other things.""And that virus is present in the body secretions and solutions that people may come in contact with," he adds. "And usually, the body is still quite warm, and the virus is still living."The virus can remain infectious as long as bodily fluids remain moist.On a molecular level, Plachter notes that viruses are stable structures that persist in fluid environments:"If somebody dies, there is enough fluid still available, so the virus is stable inside the body."This makes funeral practices particularly risky in the early post-death period, when viral loads remain high.What comes next in the outbreakContainment is challenging. Population movement can spread the virus across borders, while traditional burial practices can increase exposure.Heymann explains: "It will be very difficult to stop because of the mobility of people, because of the misunderstanding about burial and the violence that's occurring, because of civil war, and because of just lack of trust of the people in the area of outsiders."Safe burial practices exist, including protective equipment and controlled handling of bodies, but require trust and community cooperation.History shows containment is possible. In 1977, Congo’s second recorded Ebola outbreak was stopped after early detection and isolation of a patient, preventing further spread.However, the current outbreak is more complex, occurring in areas affected by conflict and population movement.Research is also limited, as Ebola can only be studied in high-level biosafety laboratories, restricting real-time understanding of this strain.Experts emphasize early detection, infection control, and community engagement — but achieving all three simultaneously remains difficult in the present context.Bundibugyo Ebola: vaccines and treatments still limitedThis outbreak involves the Bundibugyo strain, against which existing vaccines are not confirmed to be effective. Current approved Ebola vaccines, including Merck’s Ervebo and others targeting the Zaire strain, were designed for different variants.The World Health Organization is considering whether to deploy Ervebo despite limited evidence of effectiveness against Bundibugyo.There are currently no approved treatments for this strain.However, research is ongoing. Oxford University and India’s Serum Institute are developing a vaccine using COVID-era platform technology, with human trials potentially beginning within months.In addition, scientists in China are testing an experimental mRNA vaccine designed to target multiple Ebola strains, including Bundibugyo.Even so, experts caution that effective vaccines and treatments may still be months or years away.Read: WHO Chief Arrives in Congo Amid Ebola Outbreak
What You Need to Know About the New Ebola Outbreak in Congo
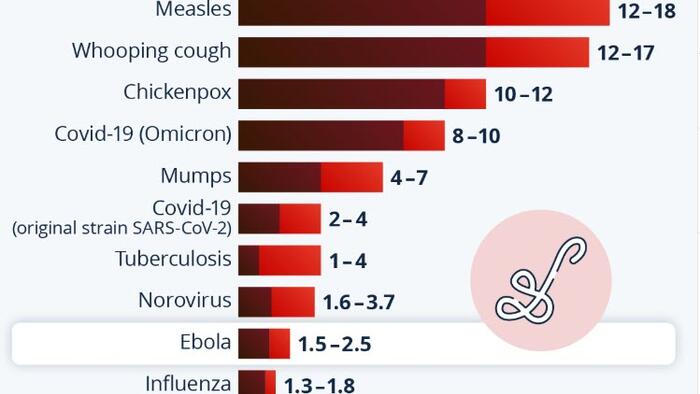
The virus spreads through direct person-to-person contact and can remain highly infectious in corpses, making funeral practices especially dangerous.
TL;DRAI
A Bundibugyo Ebola outbreak is spreading in DRC with no effective vaccine or treatment — approved options target only the Zaire strain. Oxford and Chinese teams are advancing mRNA multi-strain Ebola vaccines on COVID-era platforms, with human trials months away.
878 words~4 min read