Notes on architecture, licensing landmines, and why I'm building offline-first medical AI for community health workers — not radiologists.
Why this exists
There is no shortage of medical AI startups, and almost all of them are building for the same user: a radiologist or pathologist working in a well-resourced hospital with cloud connectivity, an electronic health record, and the budget to license a SaaS dashboard. That market is real, but it's also crowded, slow to adopt, and over-served.
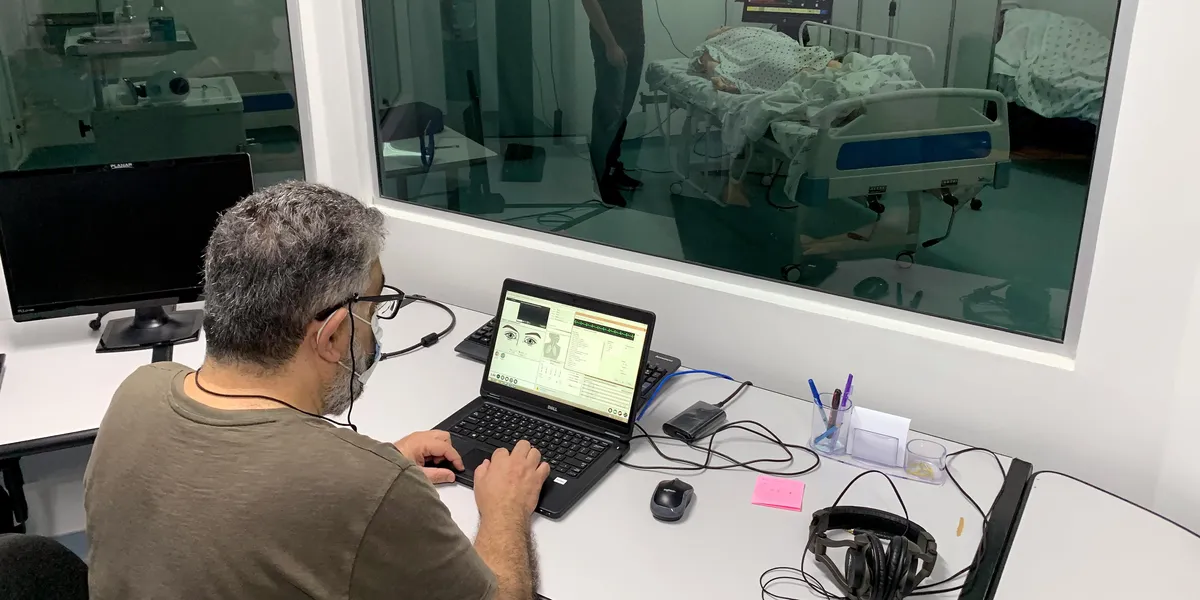
The user I care about is different. She is a Community Health Extension Worker — sometimes called a CHEW — working in a district clinic in sub-Saharan Africa, often the only clinical-grade contact a village has with the formal health system. She does not have an internet connection during the visit. She is the screening layer, the referral decision, and the patient education function all in one role. Her tools are her training, a smartphone, and whatever cheap peripherals she can carry in a shirt pocket: a digital stethoscope, sometimes a $400 smartphone-mounted fundus adapter, occasionally a portable ultrasound probe.
This is the deployment context that should shape medical AI architecture. It mostly doesn't.