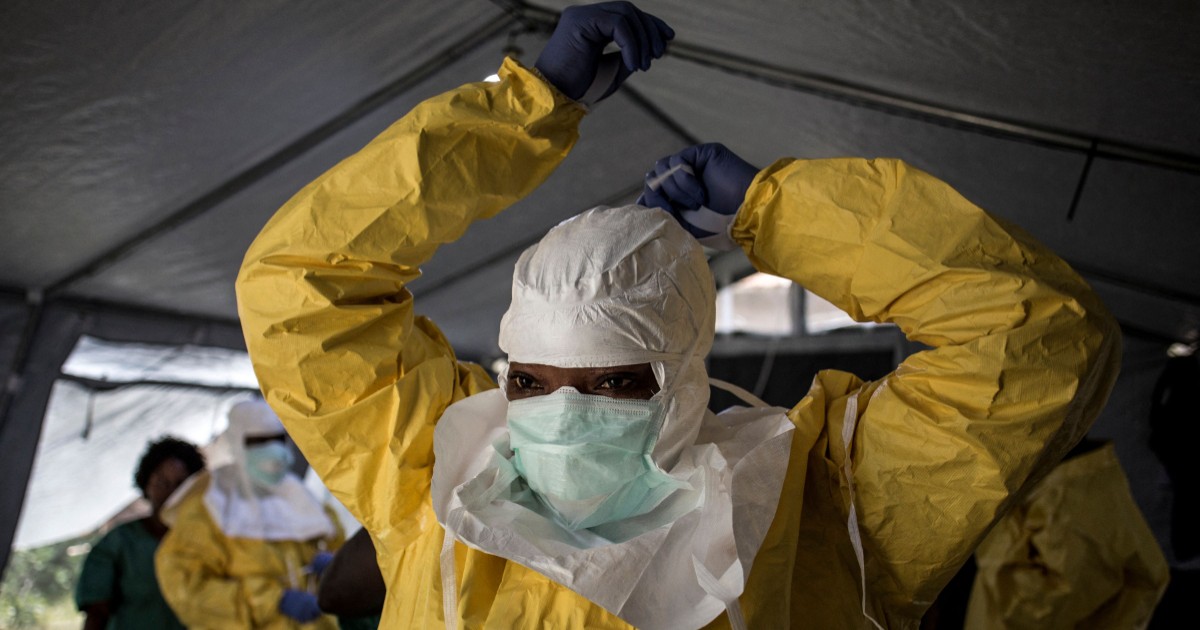
In central Africa, the number of Ebola cases is rising every day. The outbreak is centered in the eastern regions of the Democratic Republic of Congo, but this rare strain of Ebola is also spreading, from the Ituri province in the north, to the south. It even reached Kampala in neighboring Uganda. At least 139 deaths are suspected to be the result of the outbreak. A woman mourns her child, who died of Ebola, at the General Hospital in Bunia, Congo, Thursday, May 21, 2026. Moses Sawasawa/APTo learn more, The World’s Host Marco Werman spoke to Armand Sprecher, an emergency physician and epidemiologist with Doctors Without Borders, and has worked directly on Ebola responses in West and Central Africa, helping to run outbreak treatment centers and surveillance operations.Marco Werman: So, Armand, what’s different about Ebola this time around? Armand Sprecher: Our starting point is later than we would like. Usually, we come into contact with these outbreaks when the number of deaths is in the handfuls and the number of cases is in the dozens … and we are behind the game here. There’s hundreds of suspected cases, a large number of deaths, and probably most alarmingly, a significant amount of geographic spread. You know, small outbreaks become big outbreaks because people move, and people have already started to move, and we’ve had cases show up in Kampala, Uganda, and all along the eastern border of the Congo. So it is a worrying start because we’re just getting set up. Addressing this is already behind the eight ball. This is a lethal disease, and it is a rare form of Ebola. So, in terms of people’s fears, does the outbreak feel different from what you recall in 2014 in West Africa? There’s always a lot of fear [around] these viruses and outbreaks. Probably the most difficult [aspect] of having a virus we haven’t seen in a long time is that the tools we’ve become accustomed to [using] don’t work. The medicines that we have had for Ebola for some years now, on the vaccine, are designed to treat the Ebola virus that happens so often in the Congo, and when this one shows up, they’re not going to work for us. Now there are investigational therapeutics we’re going to try. We have great faith that they will do as well as the previous ones, but until we show that with a clinical trial, we’re not gonna be able to use them widely; so, we’re gonna get started, cross your fingers and move forward.Workers load World Health Organization (WHO) emergency supplies onto a United Nations plane in Nairobi, Kenya, Wednesday, May 20, 2026, headed for Congo to combat the Ebola outbreak in Ituri province. Andrew Kasuku/APWe have heard health officials describe the confirmed cases as potentially just the tip of the iceberg. Are you seeing any indicators that make you worry this outbreak is much larger than current estimates suggest? Well, it’s hard to know, but the worrying thing is that we don’t have any grasp of the chains of transmission at this stage of the game. Once you’re on the ground and have a chance to find out where the cases are, who got infected by whom, where the disease is spreading, and you have an idea of like, ‘Okay, given where this outbreak is going, I know where I have to pay attention and I know I have to concentrate my efforts’ … but we don’t have that yet. We just have a number of suspect patients, and we don’t know who’s infecting whom and where they’ve moved around. So our lack of intelligence about the current state of the epidemic is gonna make life difficult until we can get a handle on these things. I mean, we’re seeing a rapid spread. What does that mean for patients, for families and local clinicians? Because you’ve seen the impact on the ground before. What does it look like? This is a disease that is transmitted through friends and family when they take care of you when you’re sick, and they attend your funeral when you die. So somebody traveling by themselves, who’s on a business trip to Kampala and dies in a hospital, doesn’t really have much of an opportunity to pass it on to anyone, if the hospital’s got their infection control procedures in place. However, if they’re traveling to visit friends and families and they fall sick there, their family’s going to take care of them. They’re going to get sick. Somebody’s going to die. There’s going to be a funeral. People will come from different places to be at the funeral, and then they might get infected and go home to their families. So, it’s the travel within social networks that is the biggest source of spread. And we don’t have an eye on that right now to know what sort of travels are going on, but that’s the big worry. Seen through fence netting, a woman waits at the General Hospital where she brought her younger brother who was showing symptoms of Ebola in Bunia, Congo, Thursday, May 21, 2026. Moses Sawasawa/APSo this outbreak involves the Bundabugyo strain; there’s no vaccine for it. How much does that fact change the public health strategy and playbook? So a vaccine is very helpful in interrupting transmission. It’s also something you can do for the community. Outbreak control involves asking people to do things they would not otherwise want to do, like hand over the care of their loved ones to us in the treatment unit, allow us to help assist with the burial of the dead so it can be done safely, welcome us when we come knock on their door every day to see how they’re doing and see if anyone who was in a contact became sick. That all goes better when you can earn trust and do something for them. And so a vaccine not only helps interrupt transmission, but it is a visible sign that you are in the community doing something for them. It’s part of establishing a trust relationship that allows other things to work well. So not having a vaccine is kind of a double whammy. Yeah, and things are made even more complicated by this outbreak, as it seems to be spreading undetected in areas with mining and amid armed conflict. Why is containment in that sort of environment especially difficult? Well, because that conflict has been going on for many, many years, and people there have learned to be mistrustful of outsiders, because when you live in that kind of a conflict area, people who come from the outside rarely mean you good. And so, when we show up, mistrust is commonplace, and we have to earn that trust if we want the community to be a partner in outbreak control. So, that conflict gets you off on a bad footing…A poster raising awareness of Ebola hangs on a wall on a street in Bunia, Congo, Thursday, May 21, 2026. Moses Sawasawa/APSo Armand, if you look back at the 2014-2016 West Africa epidemic that you were involved in, what mistakes do you most hope can avoid being repeated? Getting people up to speed. I mean, that was a large outbreak that required a large workforce, which meant getting people who had never done this before up to speed quickly. It means teaching healthcare providers to care for people safely, because we have to wear that strange protective gear that keeps healthcare workers safe; using it, working in that environment, putting it on and taking it off properly. All of that is a new skill. The vigilance required to make sure you are protected is something people learn as well. The cleaners who go through there and mop the floors with chlorine solutions that kill viruses that’ve gotten out into the open, you know, they have to be able to protect themselves as well to keep that environment safe so that other patients who come in do not become infected. Because sometimes people come in, they look like they have Ebola, but they don’t actually have it. The test is negative, and we let them go, and we don’t want them to acquire the disease while they’re in the treatment unit. So we have to keep the environment safe. We have to build special environments for that and teach people to work in them. So, you are training people and caring for the outbreak at the same time. It’s a double workload. Health workers arrive at a treatment center for disinfection exercises in Rwampara, Congo, Thursday, May 21, 2026. Dirole Lotsima Dieudonne/APWhat kind of oddity is it for locals to be, essentially, last on the news agenda in the globe, and suddenly they’re the focus of the globe? Arrival of professionals in spacesuits. That’s a part of the mistrust I was telling you about. You show up there and tell them there’s a huge problem and you have to do these things, and they say, ‘But you weren’t here a month ago. We were dying then. You know, it was things like measles and malaria, but now it’s something different, you’re telling us, and we have to listen to you? Why?’ When people come in and say, ‘This is different,’ and they say, ‘Well, it is, but … We see people sick and dying all the time, and nobody cares. Why do you care now? Are you here to make money? Are you selling our blood to pharmaceutical companies? What are you doing?’ And so we have to overcome that mistrust. So yeah, going from last to first is a source of anxiety for people. Parts of this interview have been lightly edited for length and clarity.
Ebola spread challenges global preparedness - The World from PRX
The Ebola outbreak centered in the eastern regions of Democratic Republic of Congo is expanding at an alarming rate. The new, rare Ebola variant has spread from DRC’s Ituri Province into North Kivu and the capital of neighboring Uganda. The result is more than 600 suspected cases and at least 139 suspected deaths. Armand Sprecher, an epidemiologist with Doctors Without Borders, discusses the implications with The World’s Host Marco Werman.
1,627 words~7 min read